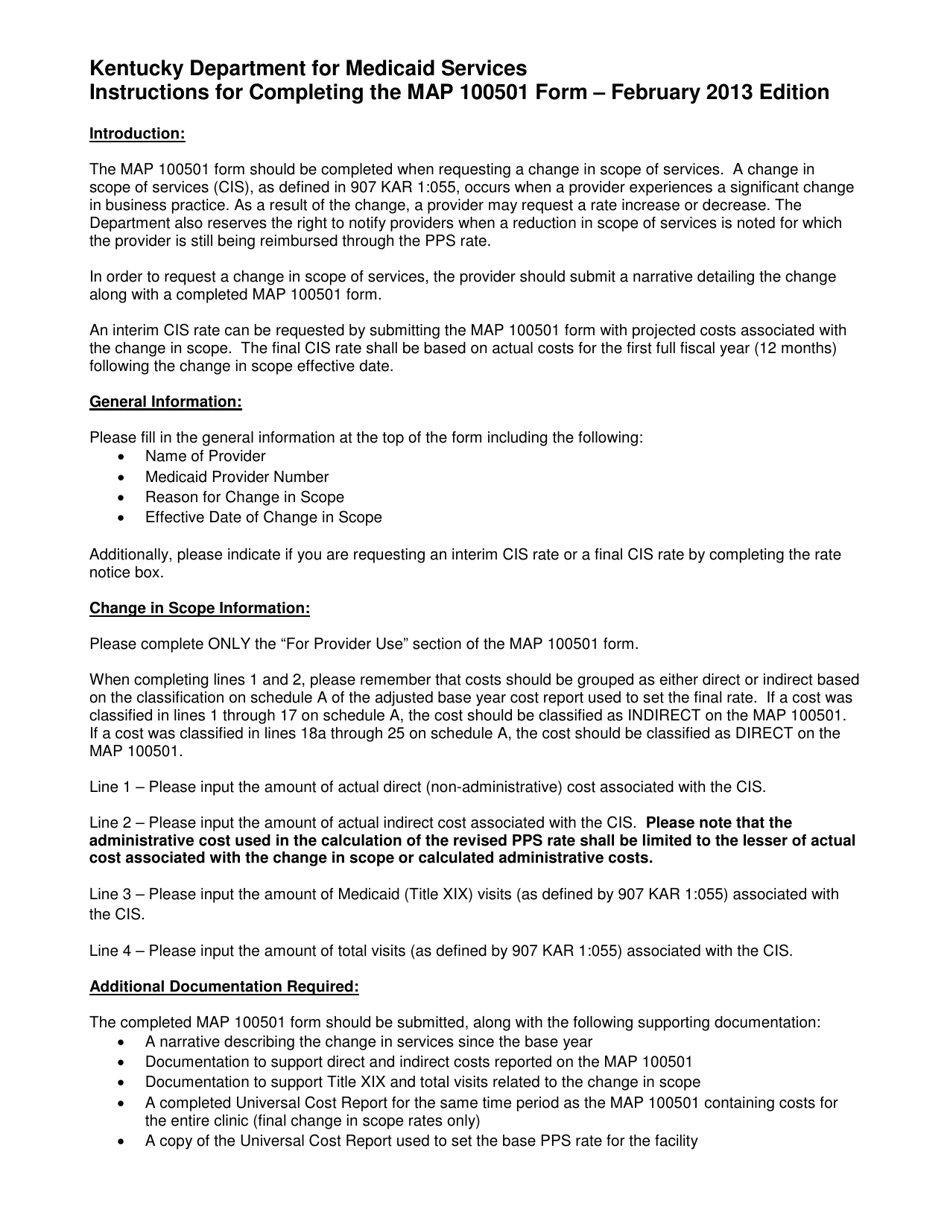
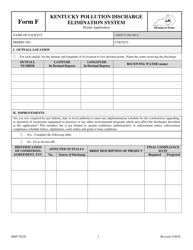
Instructions for Form MAP100501 Prospective Payment System Adjustment Form - Kentucky
This document contains official instructions for Form MAP100501 , Prospective Payment System Adjustment Form - a form released and collected by the Kentucky Department for Medicaid Services.
FAQ
Q: What is Form MAP100501?
A: Form MAP100501 is the Prospective Payment System Adjustment Form for the state of Kentucky.
Q: What does the form cover?
A: The form covers adjustments related to the Prospective Payment System.
Q: Who needs to fill out this form?
A: This form needs to be filled out by healthcare providers in Kentucky.
Q: What is the purpose of the Prospective Payment System?
A: The Prospective Payment System is designed to determine reimbursement rates for healthcare services.
Q: What type of adjustments can be made using this form?
A: This form allows for adjustments related to various factors, such as outlier payments, wage index adjustments, and low-volume payment adjustments.
Q: Is this form specific to Kentucky only?
A: Yes, this form is specific to the state of Kentucky.
Q: Are there any deadlines for submitting this form?
A: Specific deadlines for submitting this form may be provided by the healthcare department or agency in Kentucky. It is important to adhere to any applicable deadlines.
Q: What should I do if I have questions about filling out this form?
A: If you have questions about filling out the form, it is recommended to contact the appropriate healthcare department or agency in Kentucky for assistance.
Q: Is there a fee for submitting this form?
A: There may be fees associated with submitting this form. Please check with the relevant healthcare department or agency in Kentucky for more information.
Instruction Details:
- This 1-page document is available for download in PDF;
- Actual and applicable for the current year;
- Complete, printable, and free.
Download your copy of the instructions by clicking the link below or browse hundreds of other forms in our library of forms released by the Kentucky Department for Medicaid Services.