![]() This version of the form is not currently in use and is provided for reference only. Download this version of
Form C-9 (BWC-1113)
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
Form C-9 (BWC-1113)
for the current year.
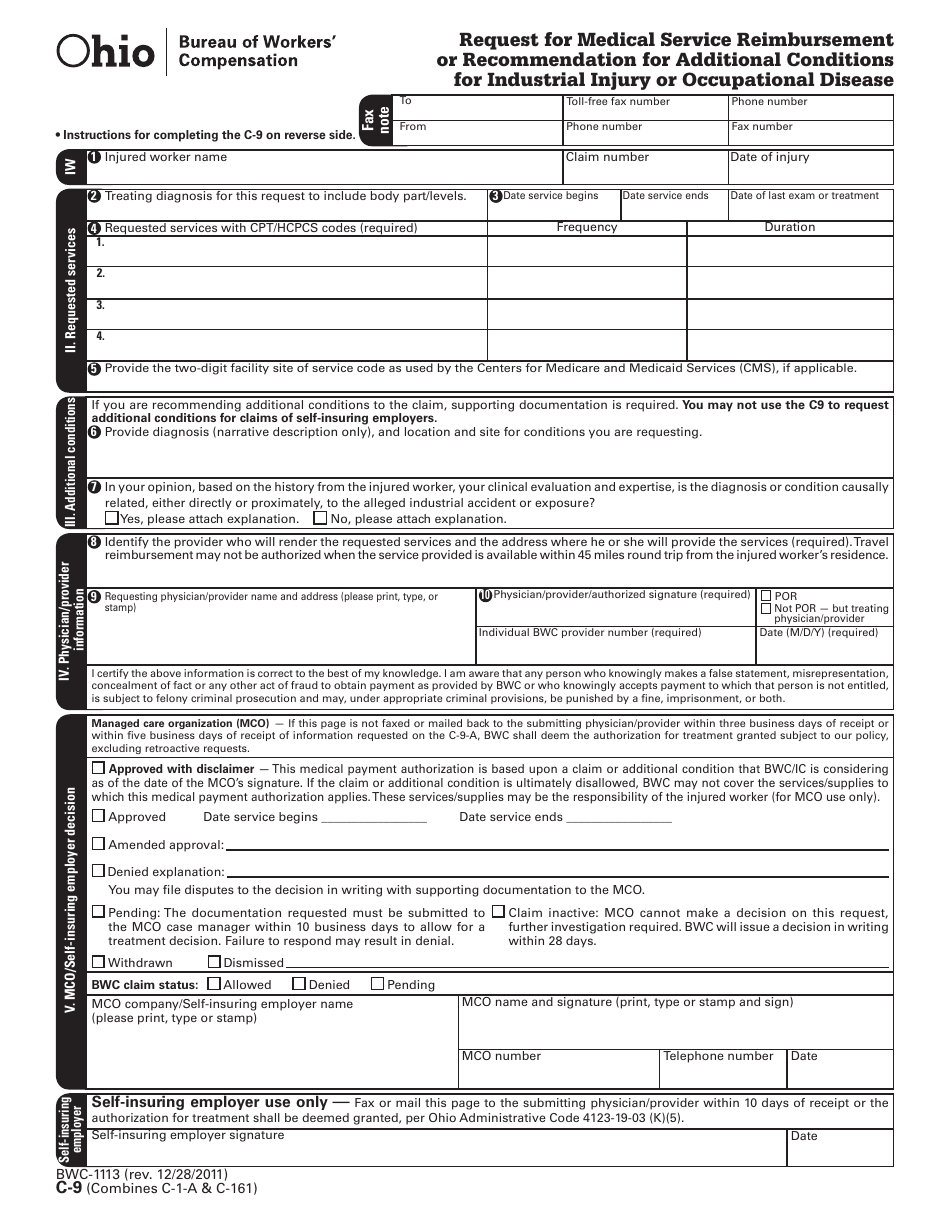
Form C-9 (BWC-1113) Request for Medical Service Reimbursement or Recommendation for Additional Conditions for Industrial Injury or Occupational Disease - Ohio
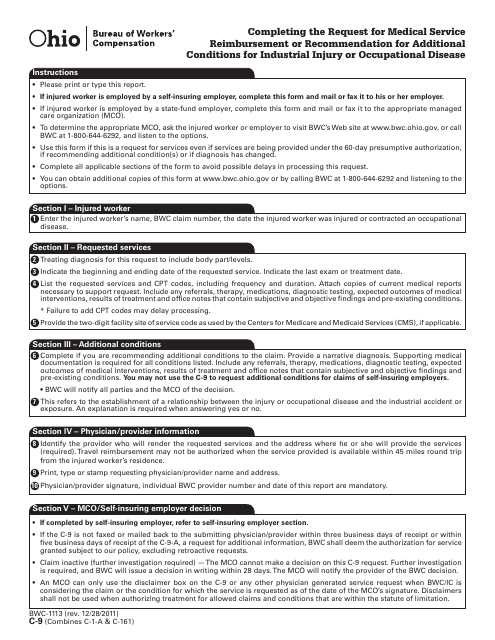
What Is Form C-9 (BWC-1113)?
This is a legal form that was released by the Ohio Bureau of Workers' Compensation - a government authority operating within Ohio. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is Form C-9?
A: Form C-9 is a document used in Ohio to request medical service reimbursement or recommendation for additional conditions for industrial injury or occupational disease.
Q: What is BWC-1113?
A: BWC-1113 is the form number assigned to Form C-9.
Q: What can I use Form C-9 for?
A: You can use Form C-9 to request reimbursement for medical services related to an industrial injury or occupational disease, or to recommend additional conditions that should be covered.
Q: How do I fill out Form C-9?
A: You must fill out the form with your personal information, details about the injury or disease, and information about the medical services or additional conditions being requested.
Q: Is there a deadline for submitting Form C-9?
A: Yes, there is a deadline for submitting Form C-9. It must be filed within one year from the date of the injury or onset of the disease.
Q: Who should I contact if I have questions about Form C-9?
A: If you have questions about Form C-9, you should contact the Ohio Bureau of Workers' Compensation for assistance.
Form Details:
- Released on December 28, 2011;
- The latest edition provided by the Ohio Bureau of Workers' Compensation;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form C-9 (BWC-1113) by clicking the link below or browse more documents and templates provided by the Ohio Bureau of Workers' Compensation.
Download Form C-9 (BWC-1113) Request for Medical Service Reimbursement or Recommendation for Additional Conditions for Industrial Injury or Occupational Disease - Ohio

1
2