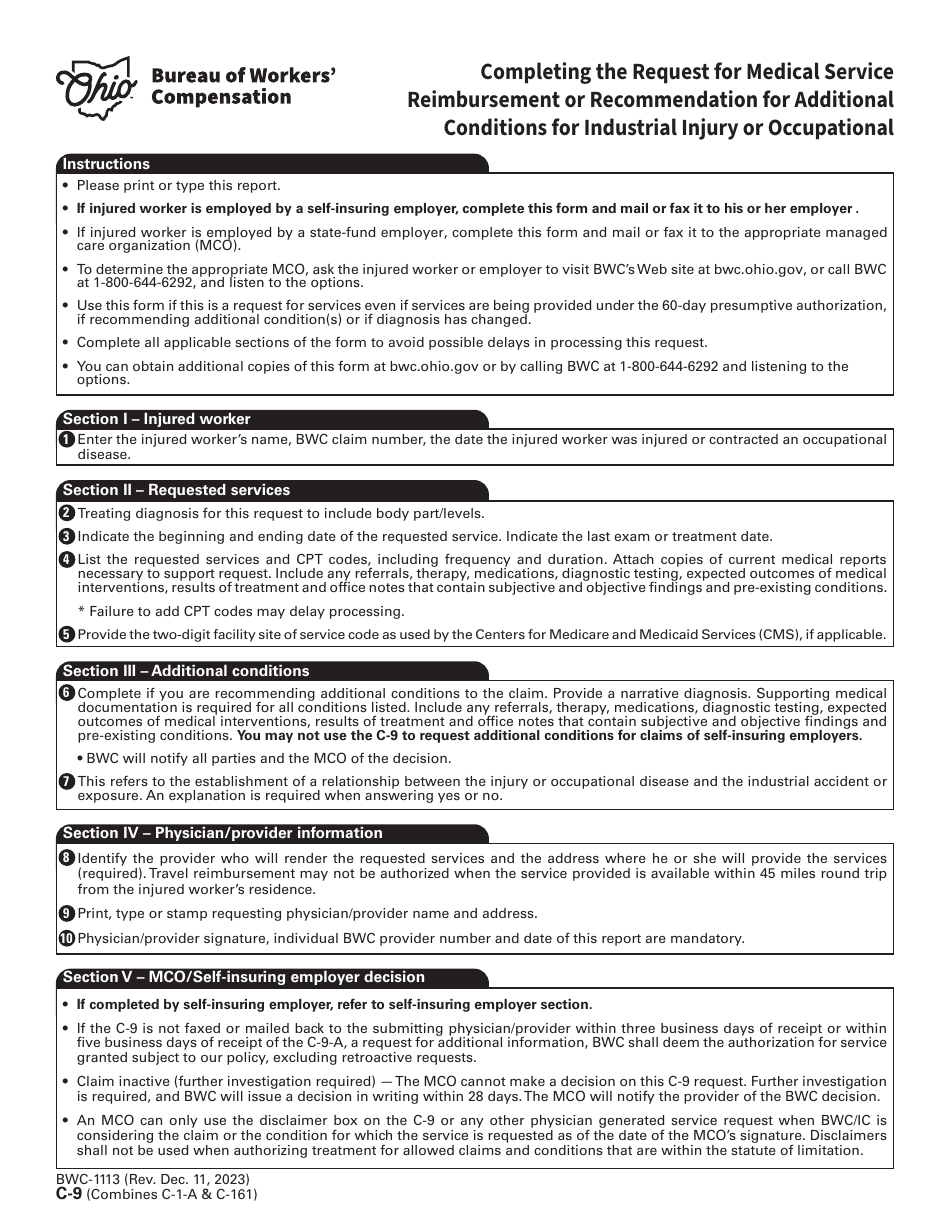
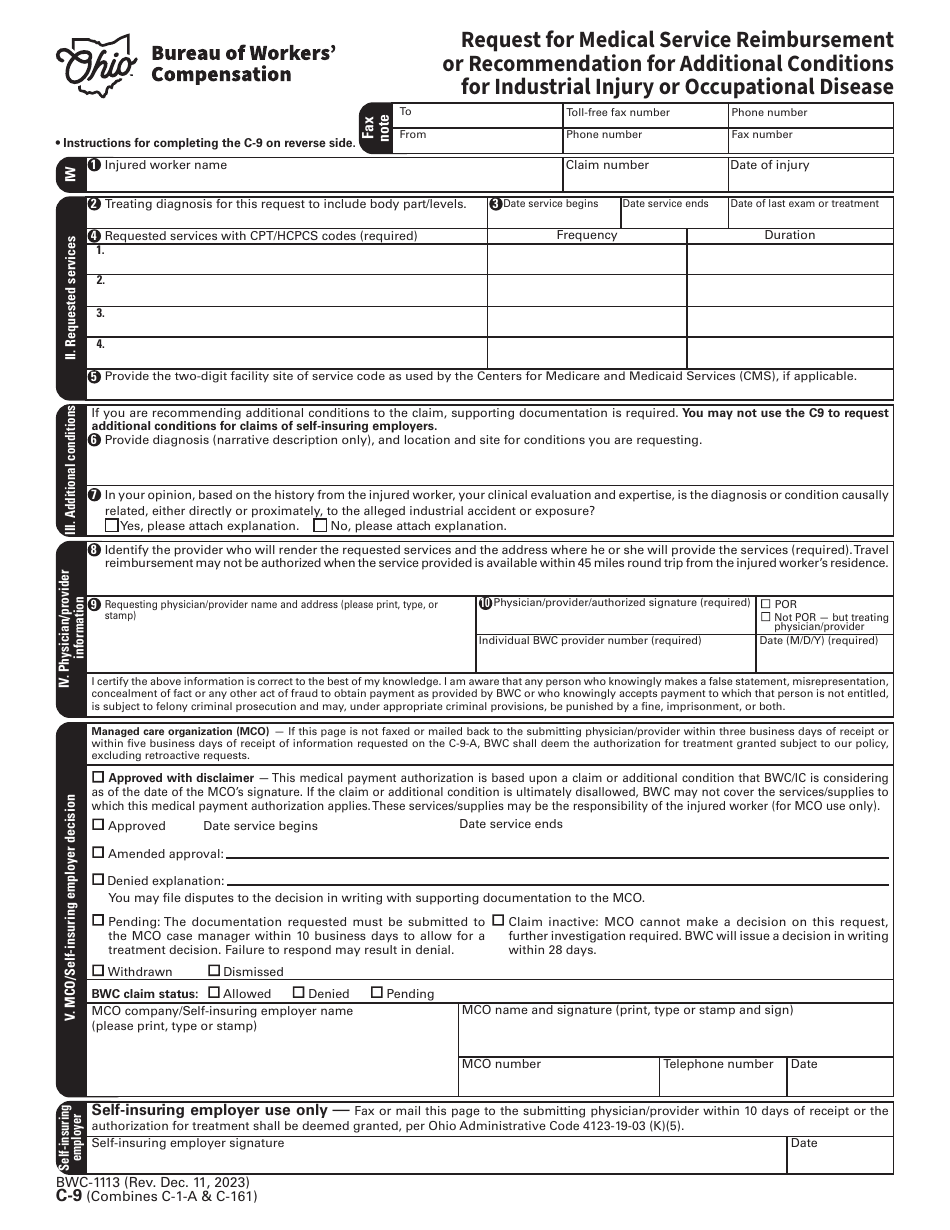
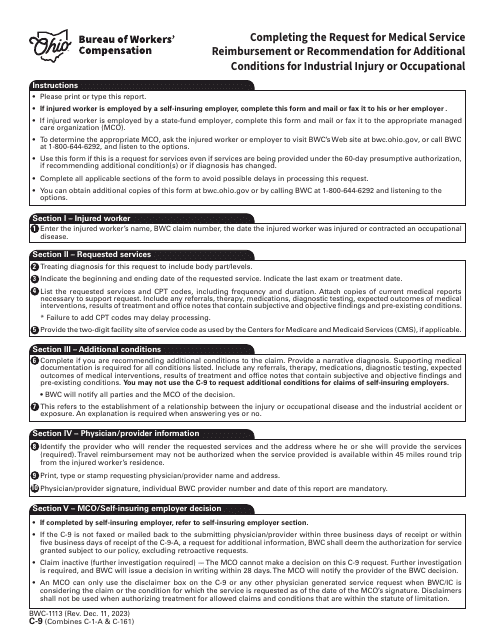
Form C-9 (BWC-1113) Request for Medical Service Reimbursement or Recommendation for Additional Conditions for Industrial Injury or Occupational Disease - Ohio
Fill PDF Online
Fill out online for free
without registration or credit card
Other Revision
Download Form C-9 (BWC-1113) Request for Medical Service Reimbursement or Recommendation for Additional Conditions for Industrial Injury or Occupational Disease - Ohio
1
2