![]() This version of the form is not currently in use and is provided for reference only. Download this version of
Form HLTH5368
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
Form HLTH5368
for the current year.
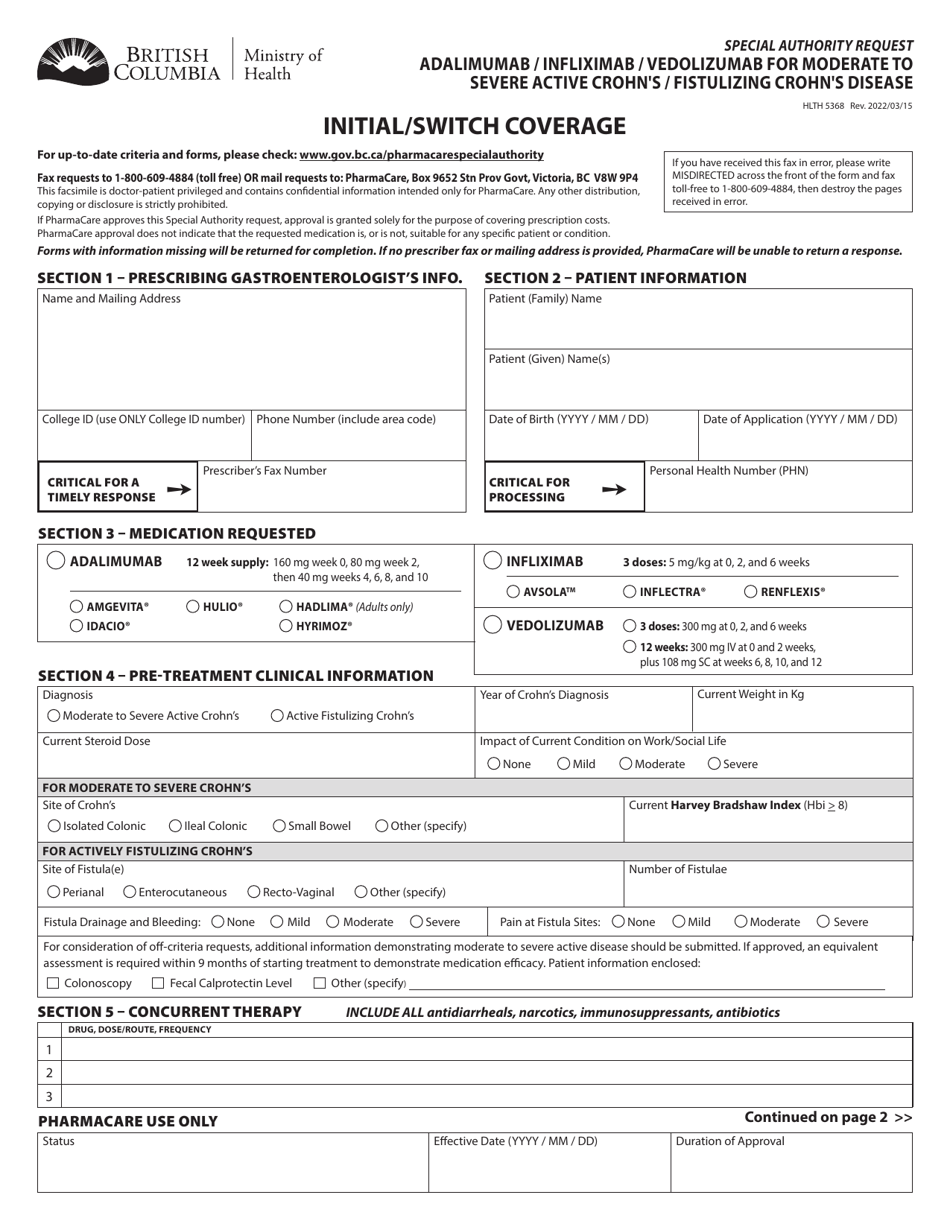
Form HLTH5368 Special Authority Request - Adalimumab / Infliximab / Vedolizumab for Moderate to Severe Active Crohn's / Fistulizing Crohn's Disease - Initial / Switch Coverage - British Columbia, Canada
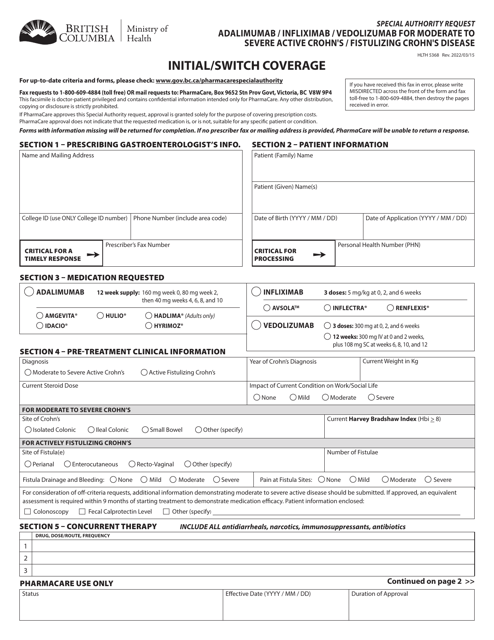
Form HLTH5368 Special Authority Request is used in British Columbia, Canada for requesting coverage of the medications Adalimumab, Infliximab, or Vedolizumab for the treatment of Moderate to Severe Active Crohn's Disease or Fistulizing Crohn's Disease. It is used for both initial coverage requests and requests to switch from a different medication.
The form HLTH5368 Special Authority Request - Adalimumab/Infliximab/Vedolizumab for Moderate to Severe Active Crohn's/Fistulizing Crohn's Disease - Initial/Switch Coverage in British Columbia, Canada is typically filed by the patient's healthcare provider or specialist.
FAQ
Q: What is the purpose of form HLTH5368?
A: The purpose of form HLTH5368 is to request special authority coverage for Adalimumab, Infliximab, or Vedolizumab for Moderate to Severe Active Crohn's/Fistulizing Crohn's Disease.
Q: Who can request special authority coverage using this form?
A: Healthcare professionals in British Columbia, Canada can request special authority coverage using form HLTH5368.
Q: Which medications are covered under this form?
A: Adalimumab, Infliximab, and Vedolizumab are the medications covered under this form.
Q: What conditions are eligible for coverage with this form?
A: Moderate to Severe Active Crohn's Disease and Fistulizing Crohn's Disease are the eligible conditions for coverage with this form.
Q: Is this form for initial or switch coverage?
A: This form can be used for both initial coverage and switch coverage.
Q: Is this form specific to British Columbia, Canada?
A: Yes, form HLTH5368 is specific to British Columbia, Canada.
Q: What is the required information to be provided on this form?
A: The required information includes patient details, healthcare professional details, diagnosis details, treatment details, and supporting documentation.
Q: Is there a fee associated with submitting this form?
A: No, there is no fee associated with submitting this form.
Q: What is the process after submitting this form?
A: After submitting this form, it will be reviewed by the Ministry of Health and a decision will be communicated to the healthcare professional.
Q: Is this form applicable for other medical conditions?
A: No, this form is specifically for Moderate to Severe Active Crohn's/Fistulizing Crohn's Disease and the mentioned medications.
Q: Can patients directly submit this form?
A: No, this form is to be submitted by healthcare professionals on behalf of the patients.
Q: Is there an expiry date for the approved coverage?
A: Yes, the approved coverage has an expiry date and may require re-authorization.
Q: What should be done in case of any changes or updates in the patient's condition or treatment plan?
A: Any changes or updates should be promptly communicated to the Ministry of Health.
Download Form HLTH5368 Special Authority Request - Adalimumab / Infliximab / Vedolizumab for Moderate to Severe Active Crohn's / Fistulizing Crohn's Disease - Initial / Switch Coverage - British Columbia, Canada
1
2