Prior Authorization Templates
Documents:
390
This Form is used for requesting prior authorization for out-of-state services in Oregon.
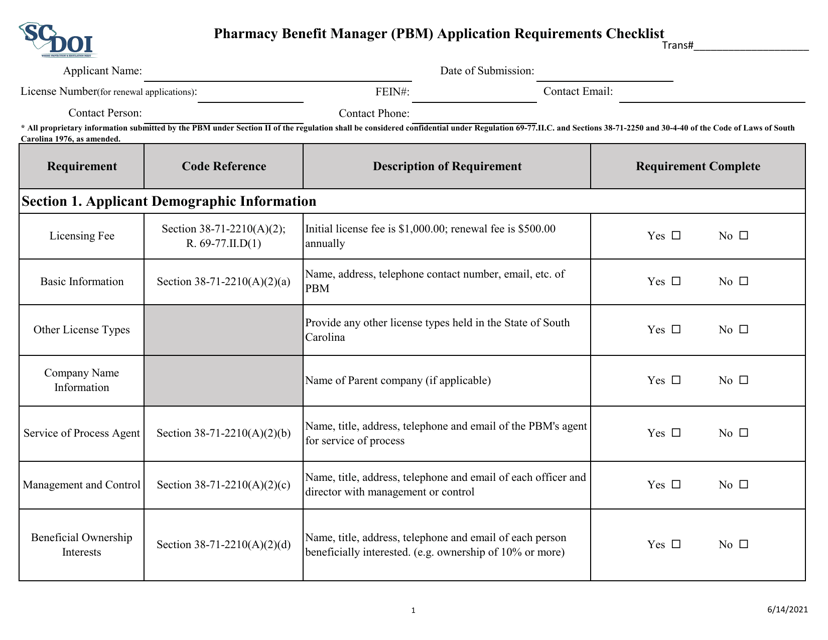
This document is a checklist outlining the application requirements for becoming a Pharmacy Benefit Manager (PBM) in South Carolina. It contains the necessary information and steps that need to be followed to apply for PBM licensure in the state.
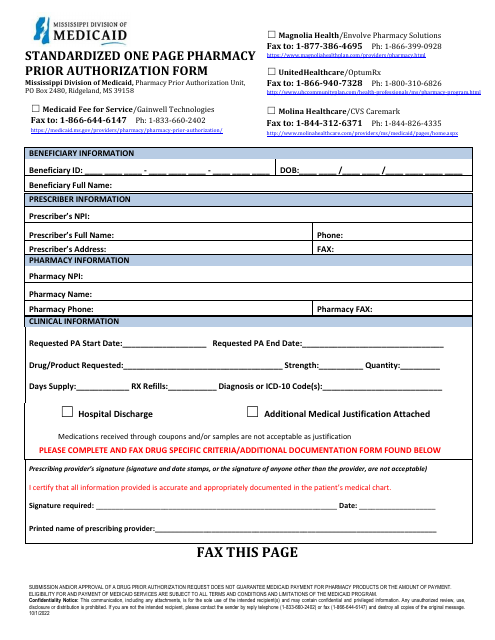
This document is used for submitting supporting documents for pharmacy prior authorization in Washington state. It serves as a cover sheet to facilitate the submission process.
This document provides instructions for completing Form F-11033 Prior Authorization/Mental Health and/or Substance Abuse Evaluation Attachment (Pa/Ea) in Wisconsin. It provides guidance on how to fill out the form and includes important information about the prior authorization process for mental health and substance abuse evaluations.
This document is used for submitting a prior authorization or care plan attachment in Wisconsin. It is required for certain healthcare services and treatments.
This document provides instructions for completing Form F-11305, which is used for prior authorization and preferred drug listing for cytokine and cell adhesion molecule antagonist drugs for Crohn's Disease in Wisconsin. It outlines the necessary information and steps to be followed when requesting approval for these medications.
This Form is used for reporting a defective prior authorization form in Washington, D.C.
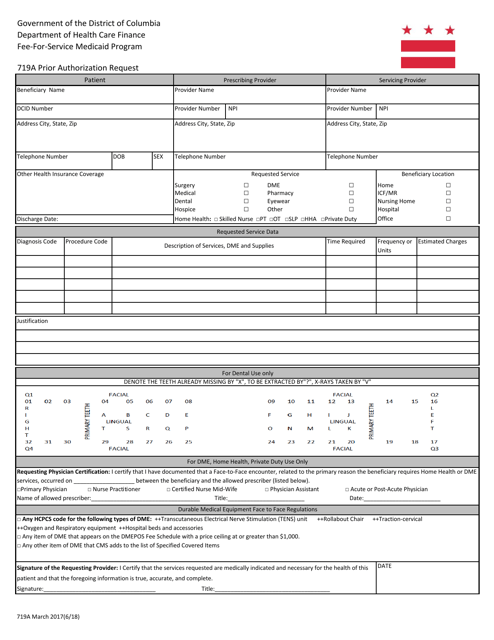
This Form is used for requesting prior authorization for medical services and treatments in Washington, D.C.
This Form is used for submitting a prior authorization request to Wisconsin's healthcare system. The fax cover sheet must be filled out and attached to the prior authorization form to ensure proper processing.
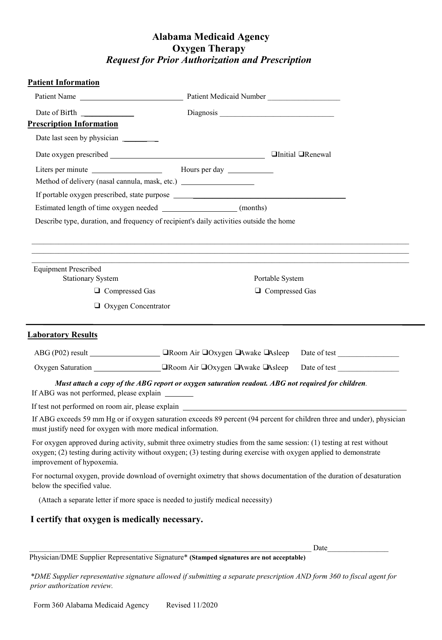
This Form is used for requesting prior authorization and prescription for oxygen therapy in Alabama.
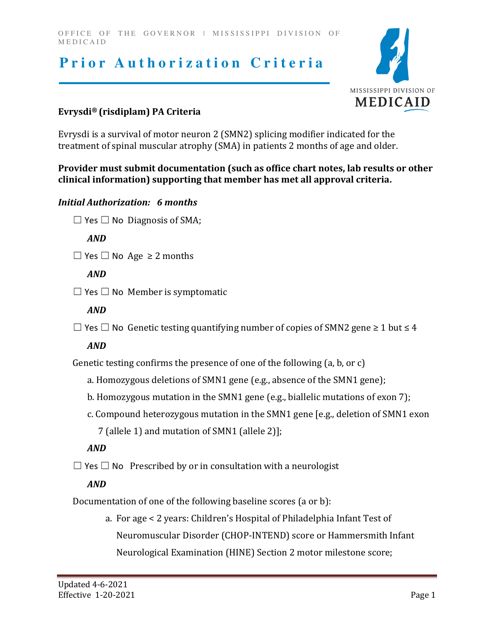
This document outlines the criteria that must be met for obtaining prior authorization for the medication Evrysdi (Risdiplam) in the state of Mississippi. It specifies the requirements that must be met in order for the medication to be approved for coverage.
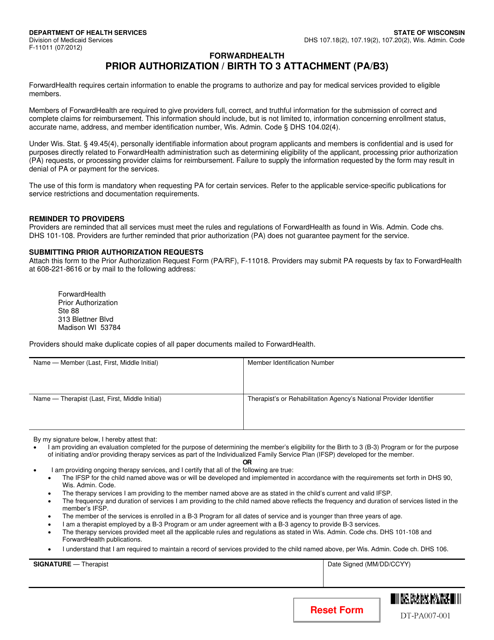
This form is used for requesting prior authorization for services related to early intervention for children from birth to age 3 in the state of Wisconsin.
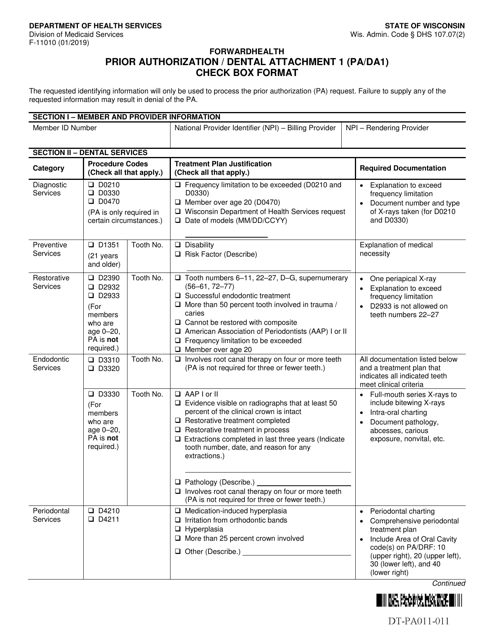
This document is used for prior authorization and dental attachments in Wisconsin. It is a check box format form.
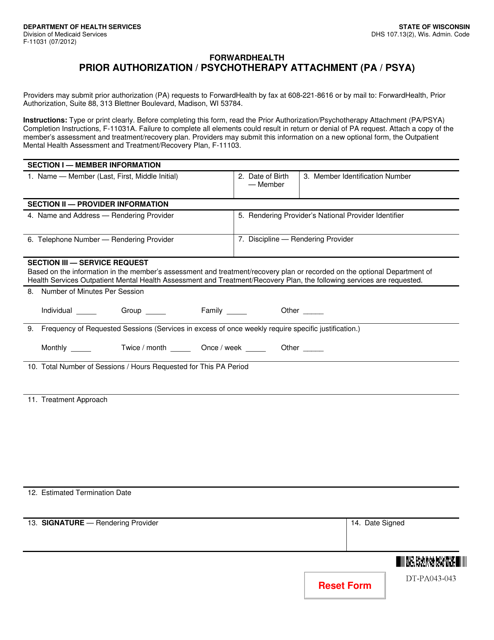
This Form is used for requesting prior authorization for psychotherapy services in Wisconsin. It is an attachment to the F-11031 Prior Authorization form.
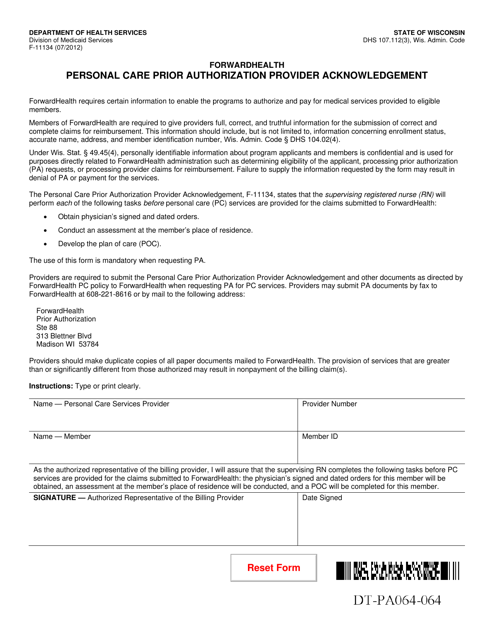
This Form is used for healthcare providers in Wisconsin to acknowledge the prior authorization request for personal care services.
