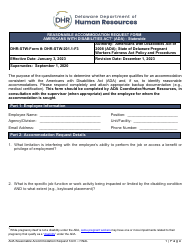
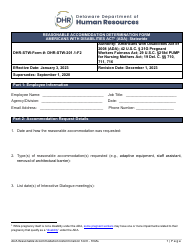
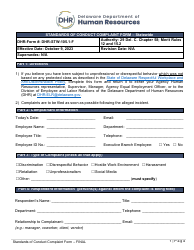
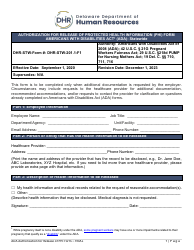
Form DHR-STW-201.1-SD1 Healthcare Provider Questionnaire in Response to an Accommodation Request - Americans With Disabilities Act (Ada) - Statewide - Delaware
Fill PDF Online
Fill out online for free
without registration or credit card
Download Form DHR-STW-201.1-SD1 Healthcare Provider Questionnaire in Response to an Accommodation Request - Americans With Disabilities Act (Ada) - Statewide - Delaware
1

2
3