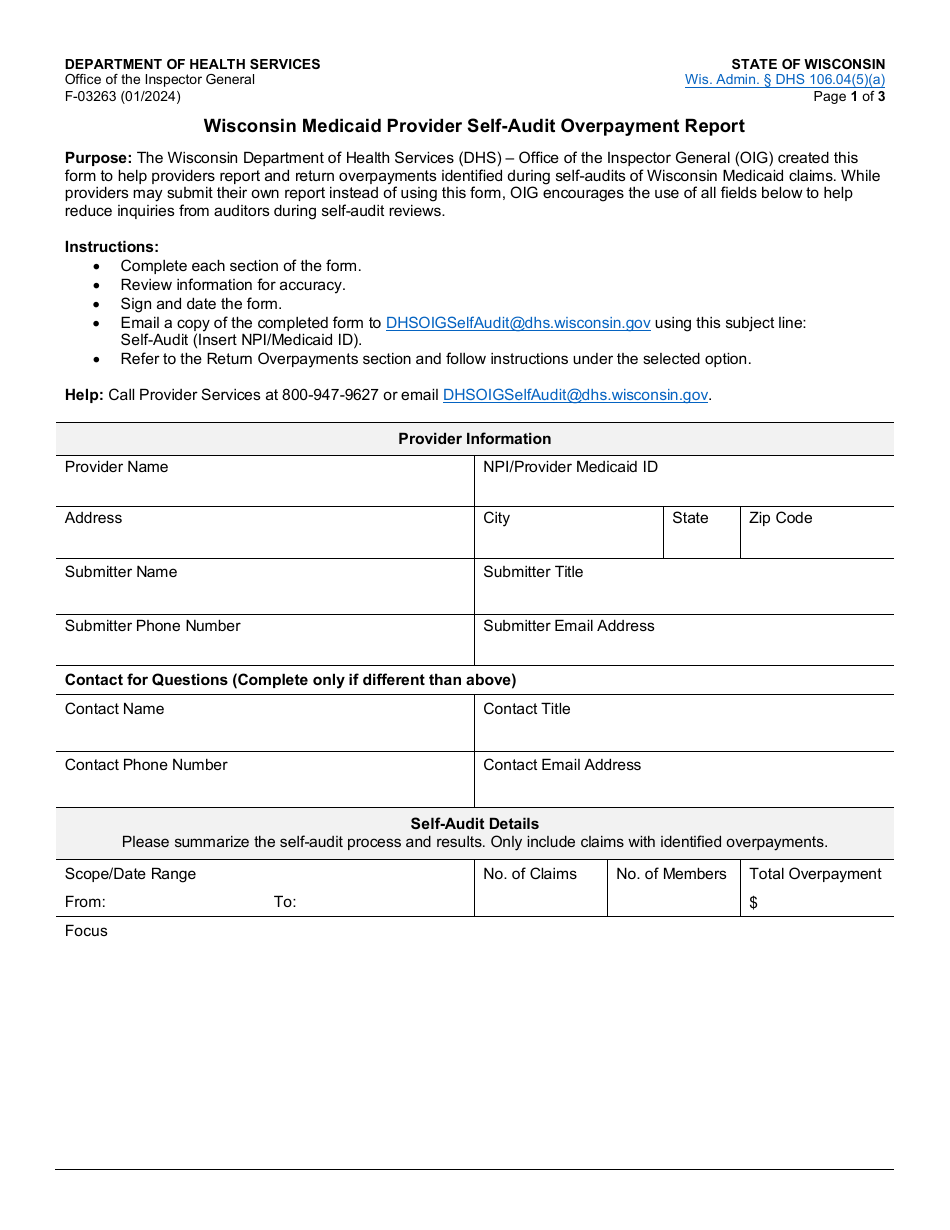
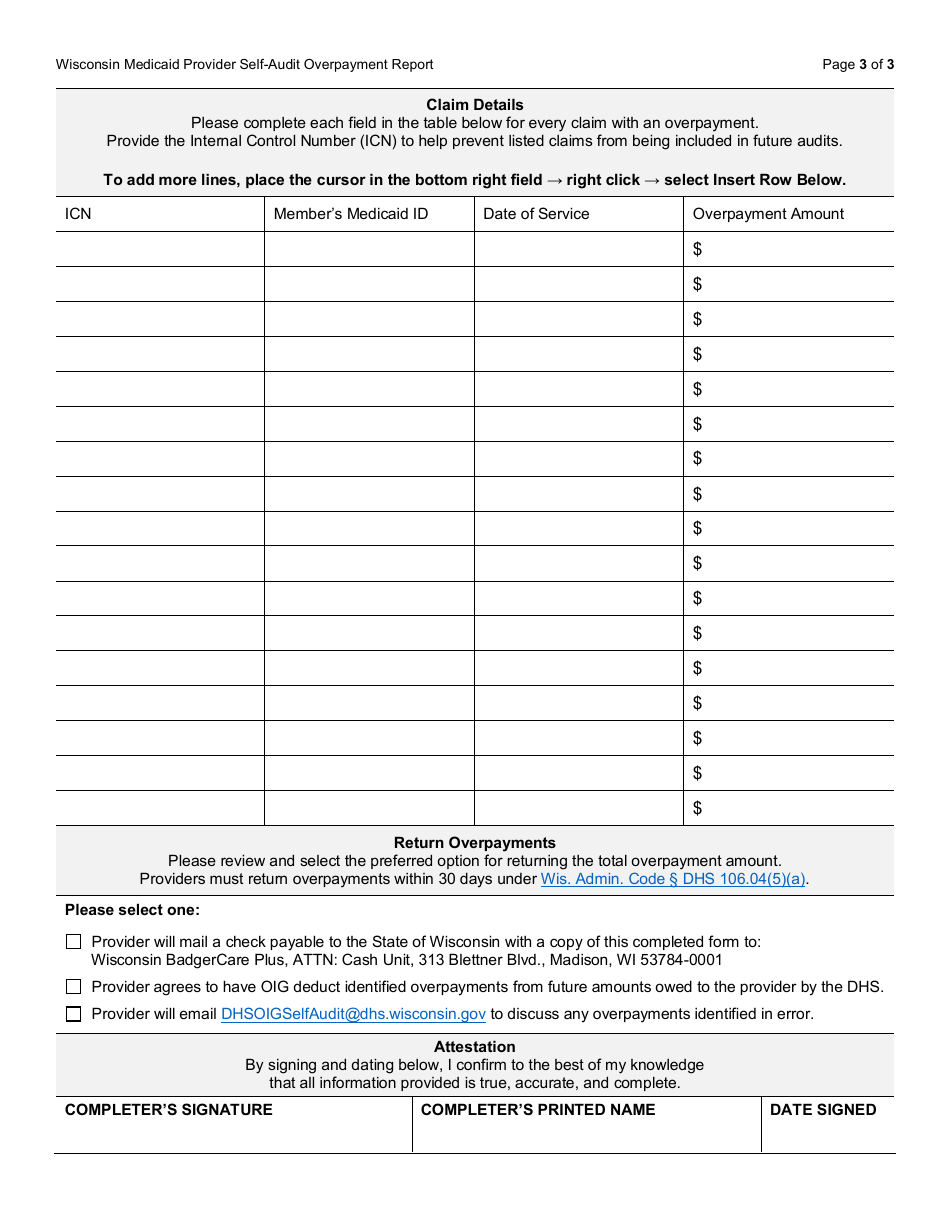
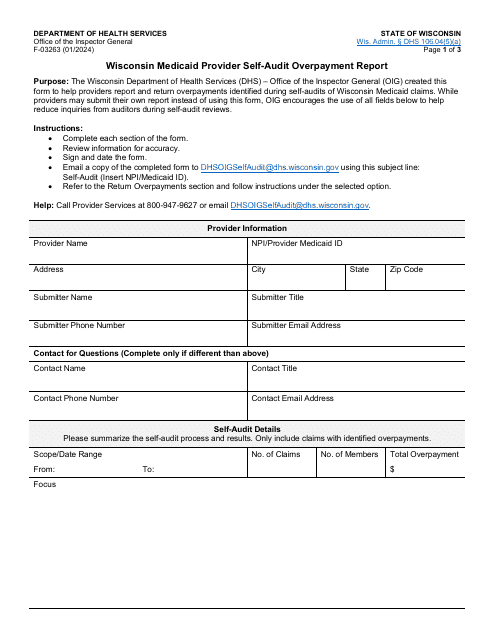
Form F-03263 Wisconsin Medicaid Provider Self-audit Overpayment Report - Wisconsin
Fill PDF Online
Fill out online for free
without registration or credit card
Download Form F-03263 Wisconsin Medicaid Provider Self-audit Overpayment Report - Wisconsin

1

2

3