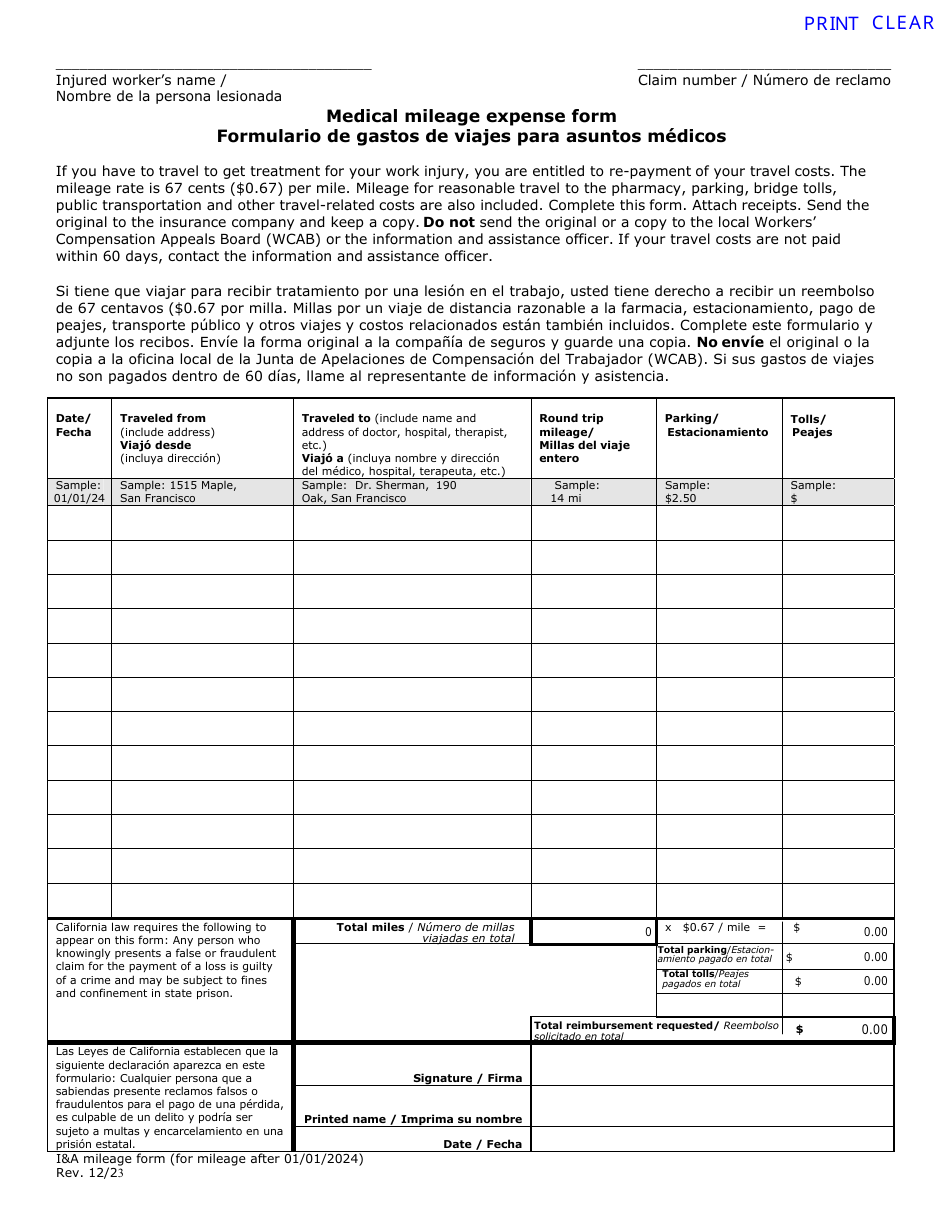
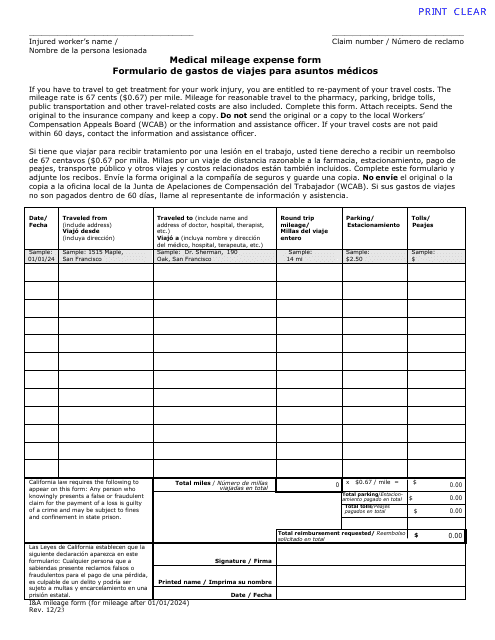
Medical Mileage Expense Form (For Mileage After 01 / 01 / 2024) - California (English / Spanish)
Fill PDF Online
Fill out online for free
without registration or credit card