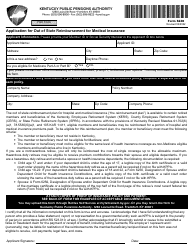
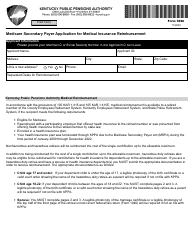
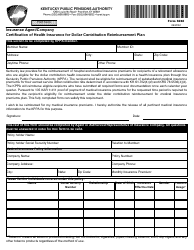
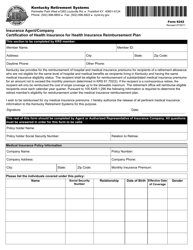
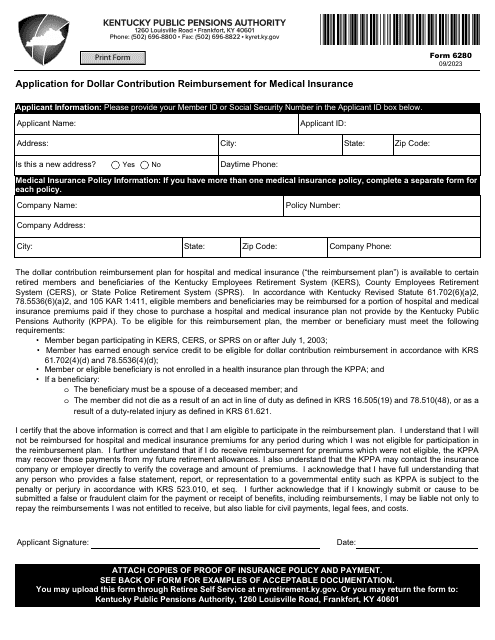
Form 6280 Application for Dollar Contribution Reimbursement for Medical Insurance - Kentucky
Fill PDF Online
Fill out online for free
without registration or credit card
Download Form 6280 Application for Dollar Contribution Reimbursement for Medical Insurance - Kentucky
1

2