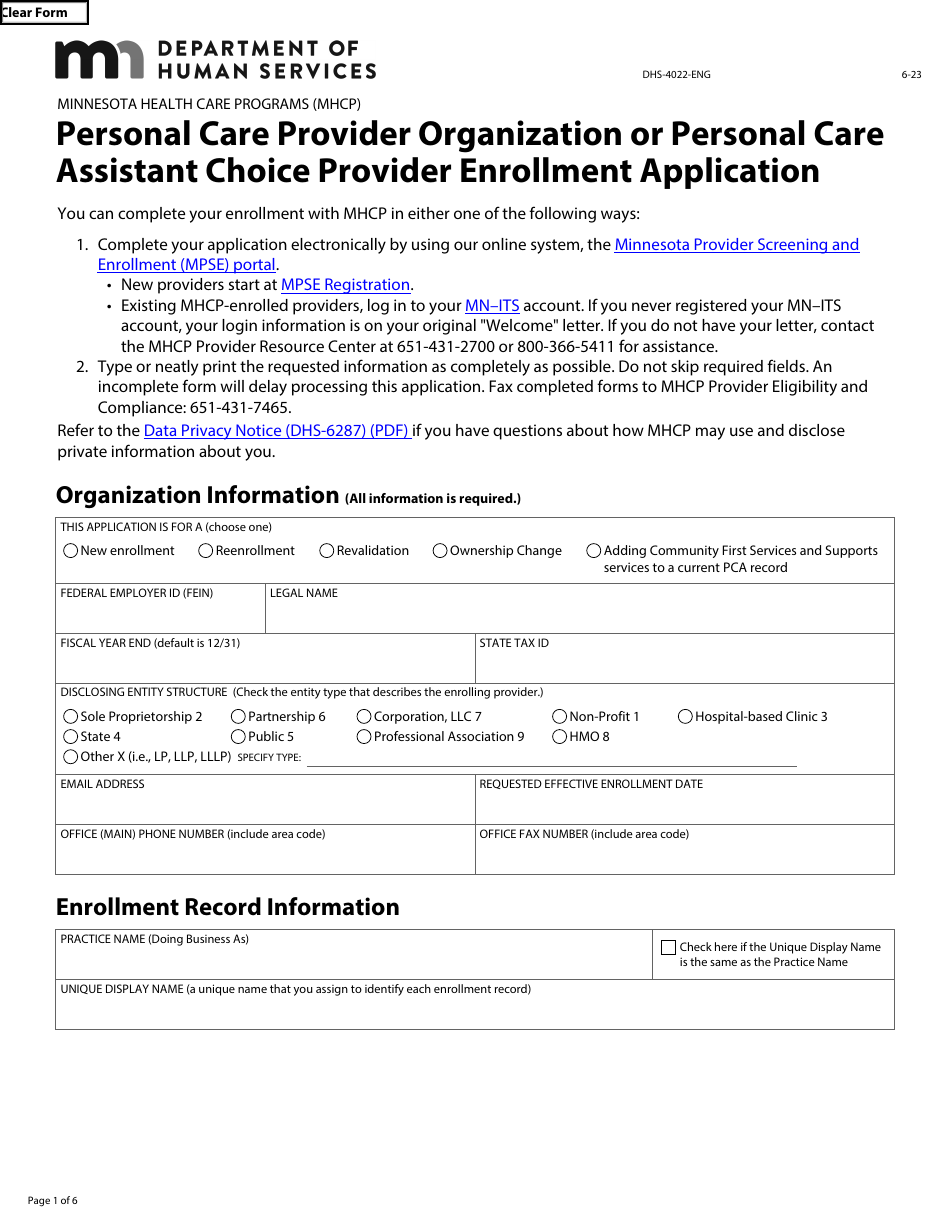
Form DHS-4022 Personal Care Provider Organization or Personal Care Assistant Choice Provider Enrollment Application - Minnesota
Fill PDF Online
Fill out online for free
without registration or credit card
Download Form DHS-4022 Personal Care Provider Organization or Personal Care Assistant Choice Provider Enrollment Application - Minnesota
1

2

3

4
5

6