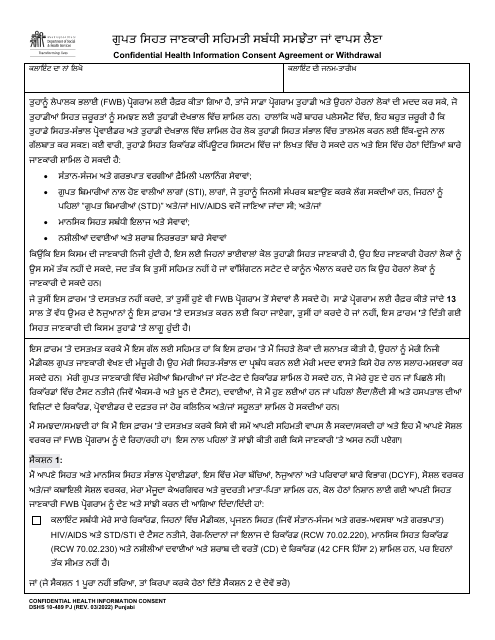
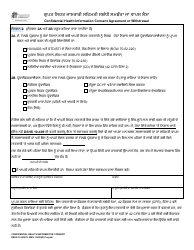
DSHS Form 10-489 Confidential Health Information Consent Agreement or Withdrawal - Washington (Punjabi)
Fill PDF Online
Fill out online for free
without registration or credit card
Download DSHS Form 10-489 Confidential Health Information Consent Agreement or Withdrawal - Washington (Punjabi)

1
2