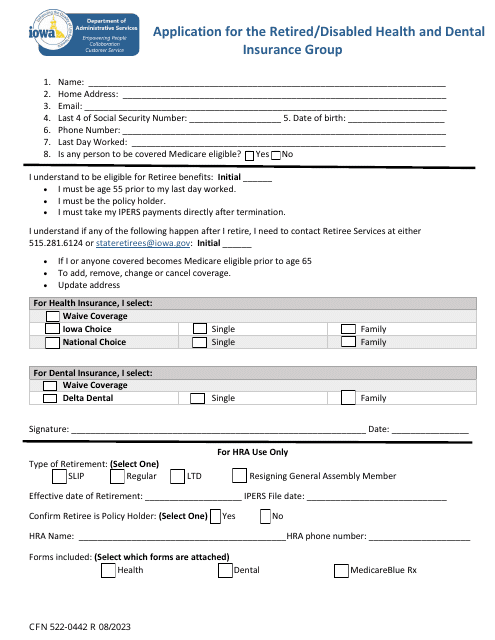
Form CFN522-0442 Application for the Retired / Disabled Health and Dental Insurance Group - Iowa
Fill PDF Online
Fill out online for free
without registration or credit card