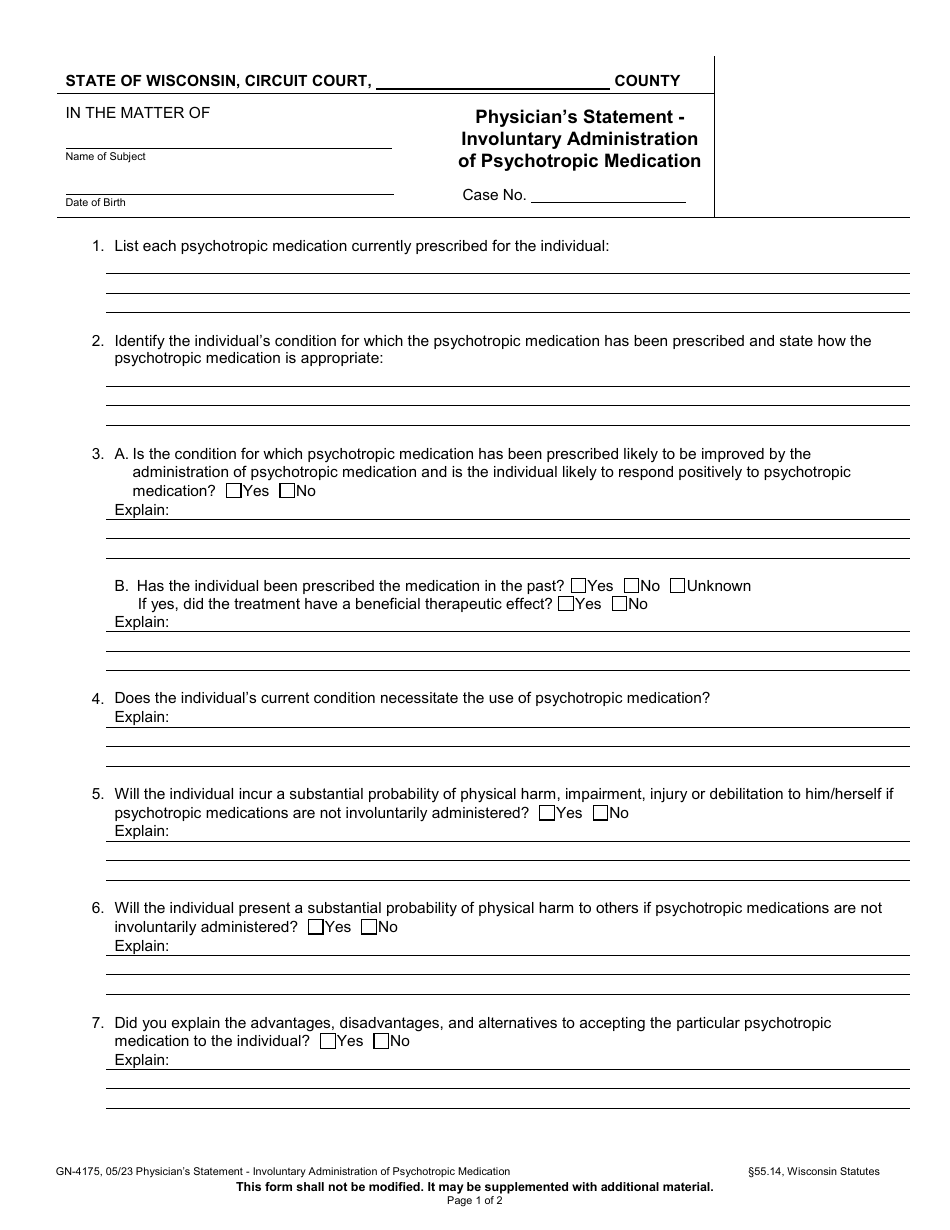
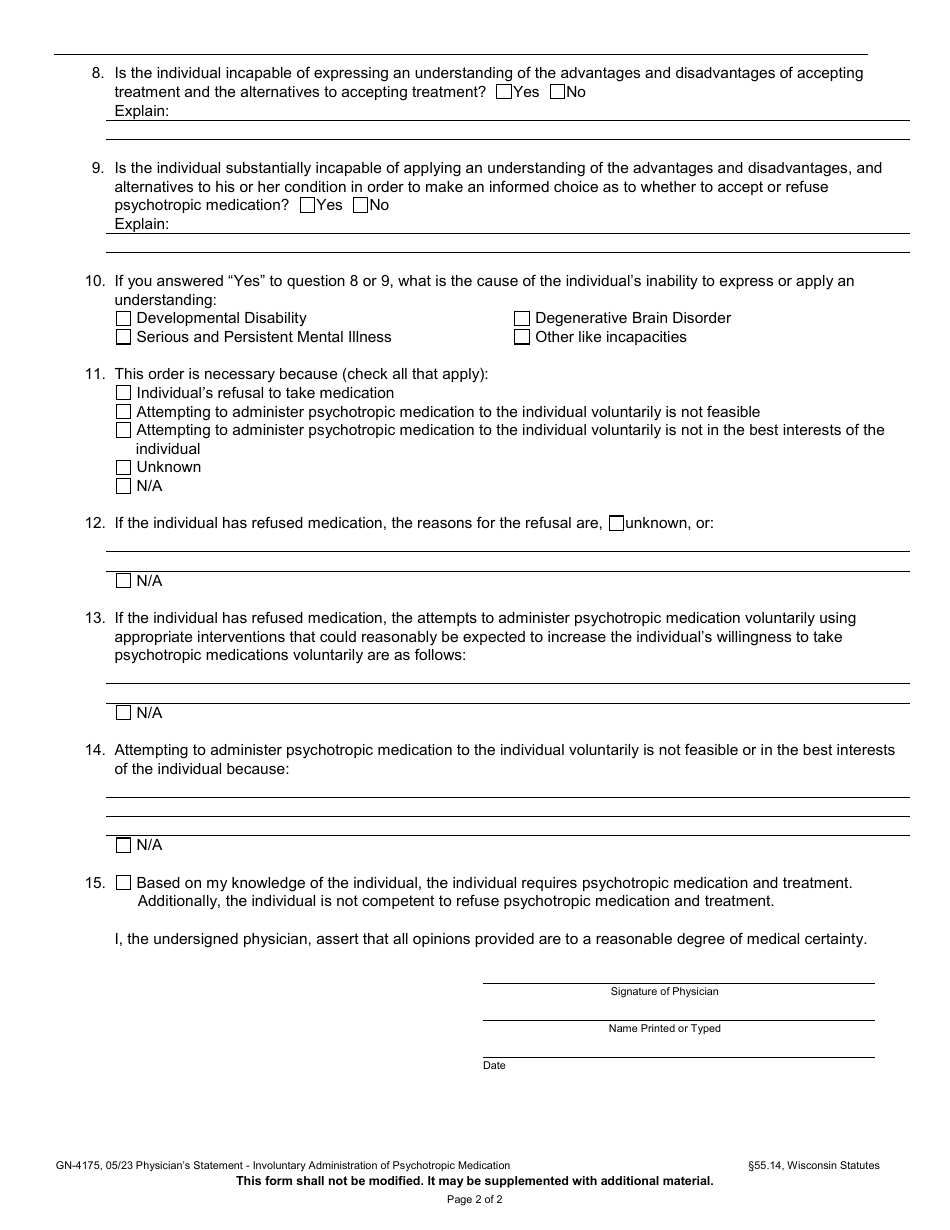
Form GN-4175 Physician's Statement - Involuntary Administration of Psychotropic Medication - Wisconsin
Fill PDF Online
Fill out online for free
without registration or credit card
Download Form GN-4175 Physician's Statement - Involuntary Administration of Psychotropic Medication - Wisconsin

1
2