Army
Business
Legal
Letters
Life
Real Estate
Tax
Wills
Blog
Upload
Medicaid Managed Care Reenrollment Member Request Form - Rhode Island
Fill
PDF
Online
PDF
Word
Army
Business
Legal
Letters
Life
Real Estate
Tax
Wills
Blog
Upload
Home
Legal
United States Legal Forms
Rhode Island Legal Forms
Rhode Island Executive Office of Health and Human Services
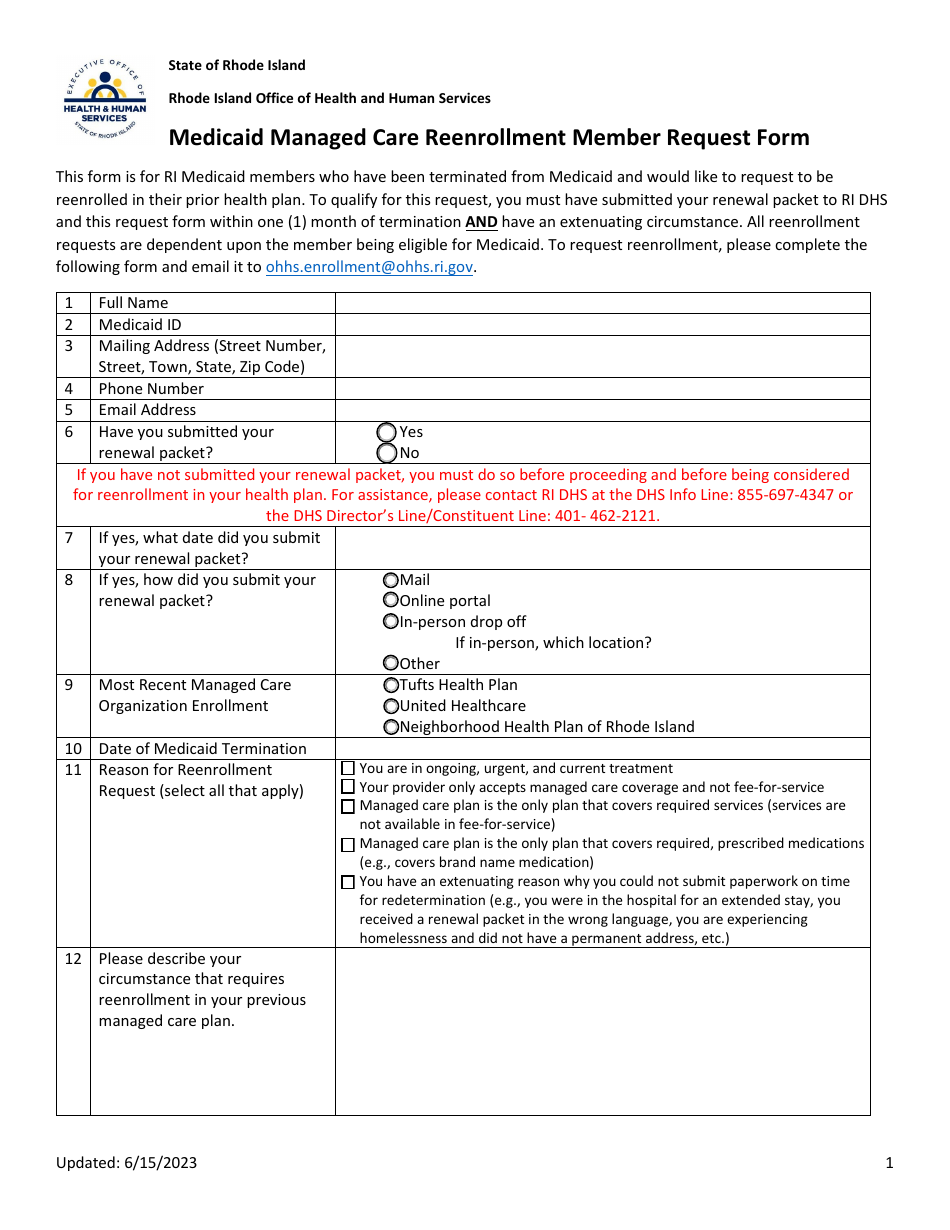
Medicaid Managed Care Reenrollment Member Request Form - Rhode Island
Medicaid Managed Care Reenrollment Member Request Form - Rhode Island
Preview
Fill
PDF
Online
PDF
Word
Fill PDF Online
Fill out online for free
without registration or credit card
ADVERTISEMENT
Download Medicaid Managed Care Reenrollment Member Request Form - Rhode Island
4.5
of 5
(
19 votes
)
PDF
Word
Fill PDF Online
ADVERTISEMENT
Linked Topics
Rhode Island Executive Office of Health and Human Services
Rhode Island Legal Forms
Legal
United States Legal Forms
Preview
Fill
PDF
Online
PDF
Word
Related Documents
Medicare and Home Health Care
Medicaid Health Plan Change Request Form - Rhode Island
Medical Immunization Exemption Certificate for Use in Health Care Facilities - Rhode Island
Appendix C Medicaid Managed Care Core Contract Attestation Statement for Mco Reporting Submission - Sample - Rhode Island
DA Form 4159 Request for Medical Care in a Federal Medical Treatment Facility Outside Department of Defense
AF Form 1466 Request for Family Member's Medical and Education Clearance for Travel
Form HCFA-605 Request for Approval as a Hospital Provider of Extended Care Services (Swing-Bed) in the Medicare and Medicaid Programs
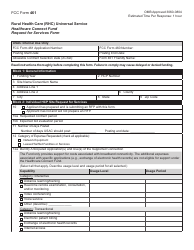
FCC Form 461 Rural Health Care (Rhc) Universal Service Healthcare Connect Fund Request for Services Form
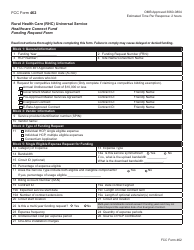
FCC Form 462 Rural Health Care (Rhc) Universal Service. Healthcare Connect Fund. Funding Request Form
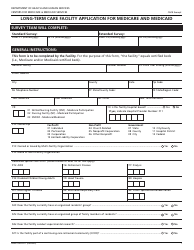
Form CMS-671 Long-Term Care Facility Application for Medicare and Medicaid
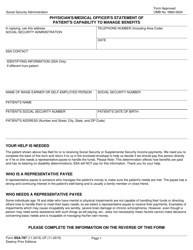
Form SSA-787 Physician's/Medical Officer's Statement of Patient's Capability to Manage Benefits
Form HCPC-FML Certification of Health Care Provider for Family Member's Serious Health Condition (Family and Medical Leave Act) - Metropolitan Life Insurance Company
Form WH-380-F Certification of Health Care Provider for Family Member's Serious Health Condition Under the Family and Medical Leave Act
Form WH-380-E Fmla Certification of Health Care Provider for Employee's Serious Health Condition
Form 61-211 Prescription Drug Prior Authorization Request Form - L.a. Care Health Plan
VA Form 10-0137 VA Advance Directive: Durable Power of Attorney for Health Care and Living Will (English/Spanish)
Cuidado Infantil Autorizado: Consultor En Atencion a La Salud - Rhode Island (Spanish)