![]() This version of the form is not currently in use and is provided for reference only. Download this version of
the document
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
the document
for the current year.
Authorization for the Disclosure of Protected Health Information - for the Purpose of Removal of Firearm Disability - Nebraska
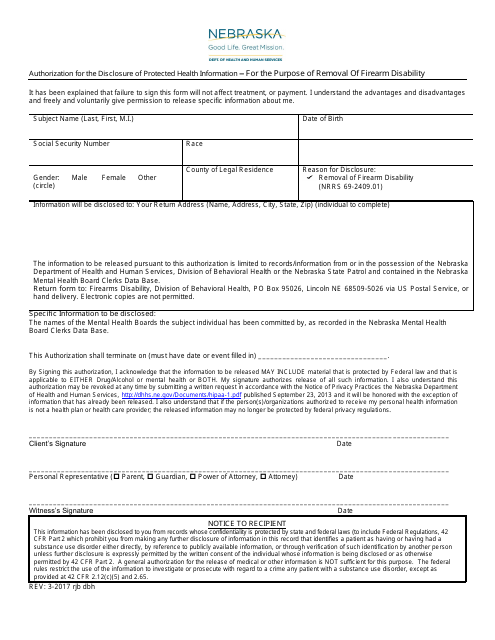
Authorization for the Disclosure of Protected Health Information - for the Purpose of Removal of Firearm Disability is a legal document that was released by the Nebraska Department of Health and Human Services - a government authority operating within Nebraska.
FAQ
Q: What is the Authorization for the Disclosure of Protected Health Information?
A: It is a document that allows the release of a person's health information.
Q: What is the purpose of the Authorization for the Disclosure of Protected Health Information - for the Purpose of Removal of Firearm Disability?
A: To remove a person's firearm disability in the state of Nebraska.
Q: Who needs to sign the Authorization for the Disclosure of Protected Health Information - for the Purpose of Removal of Firearm Disability?
A: The person seeking to have their firearm disability removed.
Q: What information is disclosed in this document?
A: Protected health information relating to the person's mental health.
Q: Is this authorization specific to Nebraska?
A: Yes, it applies to the state of Nebraska.
Q: What is the purpose of removing a firearm disability?
A: To allow a person who was previously restricted from owning or possessing firearms to regain their rights.
Form Details:
- Released on March 1, 2017;
- The latest edition currently provided by the Nebraska Department of Health and Human Services;
- Ready to use and print;
- Easy to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a printable version of the form by clicking the link below or browse more documents and templates provided by the Nebraska Department of Health and Human Services.