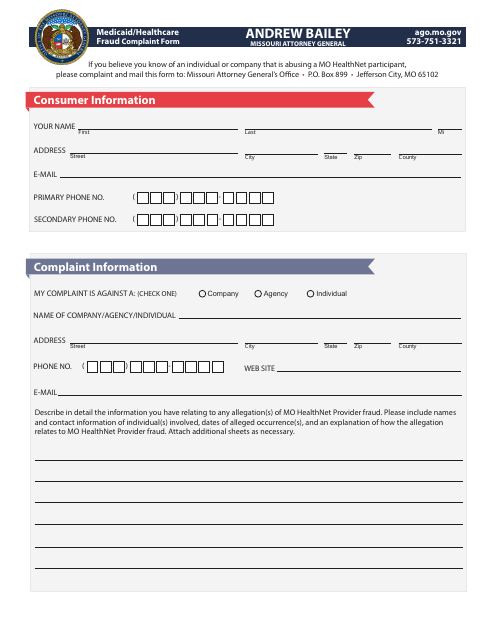
Medicaid / Healthcare Fraud Complaint Form - Missouri
Fill PDF Online
Fill out online for free
without registration or credit card
Download Medicaid / Healthcare Fraud Complaint Form - Missouri

1
2