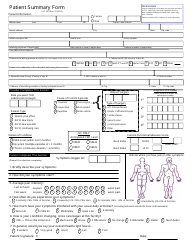
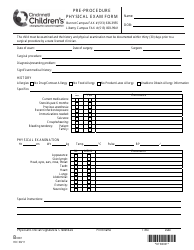
Physical Assessment Form
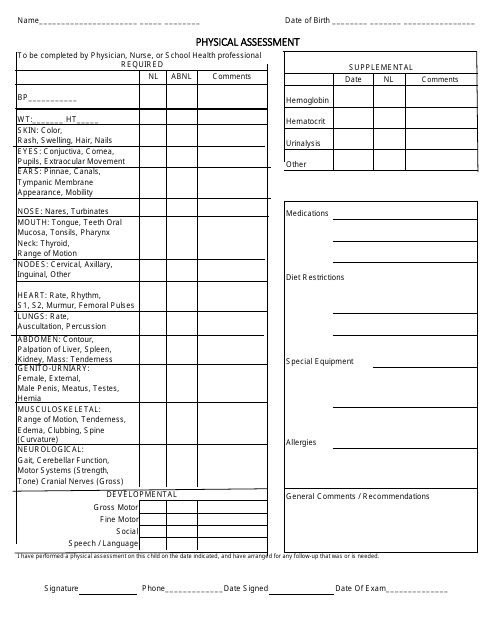
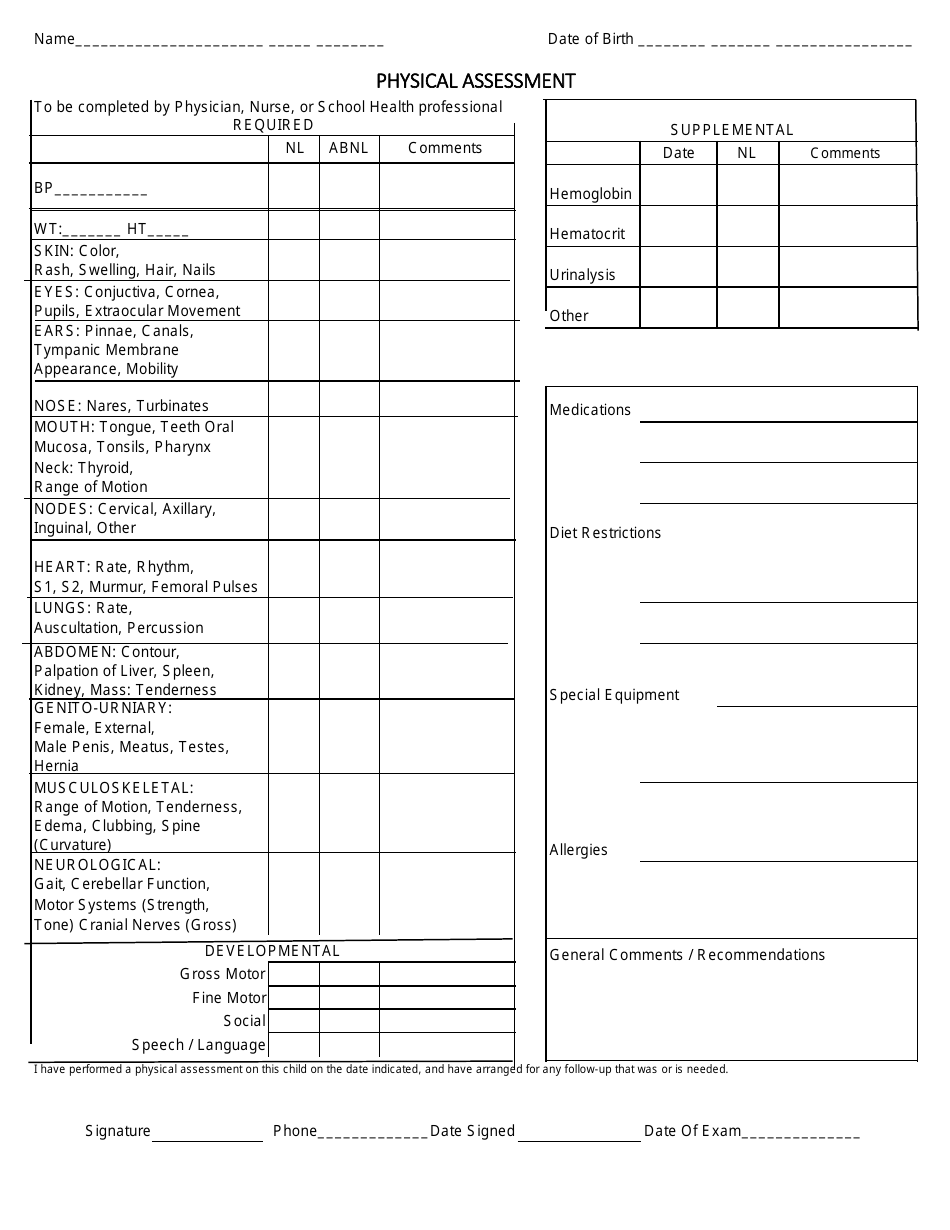
A Physical Assessment Form is a document generally used by healthcare professionals to evaluate an individual's physical health. It entails a complete physical examination which may includes checking the patient's medical history, vital signs (like pulse rate, temperature), physical features (like eyesight, mobility), organ systems (heart, lung etc.), and mental health status. This form helps to track changes in a person's physical health, identify any new or ongoing health conditions, and to guide appropriate treatment or preventive measures. It may be required for school enrollment, job or insurance applications, sports participation, or as part of routine health check-ups.
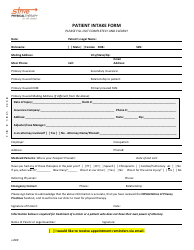
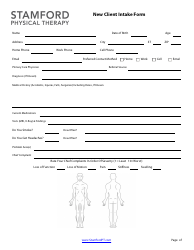
The Physical Assessment Form is typically filed by a licenced healthcare professional, such as a nurse, physician, or physical therapist. They perform a comprehensive physical examination of a patient or client and document their findings in this form. This can be done in a variety of settings like hospitals, clinics, nursing homes, or schools depending on the situation. The completed form then becomes part of the individual's medical record. These forms can be used for routine physical check-ups, or to assess an individual's health status for specific requirements such as for employment, sports participation, or insurance purposes.
FAQ
Q: What is a Physical Assessment Form?
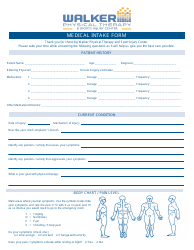
A: A Physical Assessment Form is a document that healthcare professionals use to record details of an individual's physical health. This includes information on past and present health conditions, lifestyle, vital signs like blood pressure, heart rate, and other physical parameters.
Q: Why is Physical Assessment Form important?
A: A Physical Assessment Form is important as it provides a comprehensive view of a person's physical health. It's used by healthcare professionals to identify any signs of health issues, track changes in health, and plan proper health management and interventions.
Q: Who should fill out a Physical Assessment Form?
A: Physicians, nurse practitioners, or registered nurses typically fill out a Physical Assessment Form during a physical exam or health check-up. However, parts of the form such as health history or personal lifestyle can be filled out by the patient themselves.
Q: What information is commonly included in a Physical Assessment Form?
A: A Physical Assessment Form generally includes demographic details, health history, family health history, results of a physical examination like heart rate, blood pressure measurements, and observations of physical characteristics like skin condition, mobility, posture, current medications, allergies, personal habits like diet and exercise, and any symptoms the patient may be experiencing.
Q: How often should a Physical Assessment Form be filled out?
A: The frequency at which a Physical Assessment Form should be filled out varies based on individual. It should be filled out during routine health check-ups, which for a healthy adult may be annually. However, for individuals with existing health conditions, it may need to be completed more frequently as advised by health professionals.
Q: Is the information on a Physical Assessment Form secure?
A: Yes, the information on a Physical Assessment Form is confidential and protected by law in many countries. Healthcare professionals are obligated to maintain the privacy and confidentiality of patient health information, except in certain cases specified by law.
Q: Is a Physical Assessment Form mandatory?
A: Though not mandatory, a Physical Assessment Form is essential in effectively monitoring, diagnosing, and managing a person's health. It allows healthcare providers to make informed decisions based on a comprehensive overview of the patient's health status.