Form DHS-6189K-ENG Homemaker Provider Assurance Statement - Minnesota Health Care Programs (Mhcp) - Minnesota
What Is Form DHS-6189K-ENG?
This is a legal form that was released by the Minnesota Department of Human Services - a government authority operating within Minnesota. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is DHS-6189K-ENG?
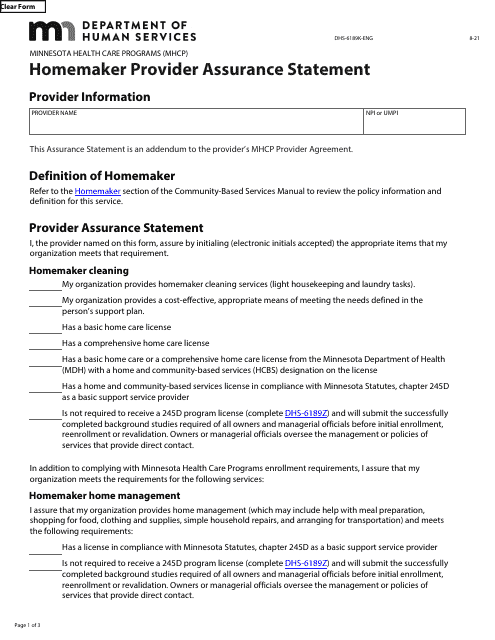
A: DHS-6189K-ENG is the Homemaker Provider Assurance Statement form used for the Minnesota Health Care Programs (MHCP).
Q: What is the purpose of the Homemaker Provider Assurance Statement?
A: The purpose of the Homemaker Provider Assurance Statement is to ensure that the provider understands and agrees to comply with the rules and requirements of the Minnesota Health Care Programs.
Q: Who needs to fill out the Homemaker Provider Assurance Statement?
A: Homemaker providers participating in the Minnesota Health Care Programs need to fill out the Homemaker Provider Assurance Statement.
Q: Do I need to submit the Homemaker Provider Assurance Statement with my application?
A: Yes, the Homemaker Provider Assurance Statement needs to be submitted with the provider's application to participate in the Minnesota Health Care Programs.
Q: What happens if I don't fill out the Homemaker Provider Assurance Statement?
A: If the Homemaker Provider Assurance Statement is not filled out, the provider will not be able to participate in the Minnesota Health Care Programs.
Q: Are there any penalties for not complying with the Homemaker Provider Assurance Statement?
A: Yes, failure to comply with the Homemaker Provider Assurance Statement may result in penalties and possible termination from the Minnesota Health Care Programs.
Q: Can I make changes to the Homemaker Provider Assurance Statement after submitting it?
A: No, once the Homemaker Provider Assurance Statement is submitted, changes cannot be made. If any changes occur, the provider must notify the Minnesota Health Care Programs.
Q: Is the Homemaker Provider Assurance Statement only applicable to Minnesota Health Care Programs?
A: Yes, the Homemaker Provider Assurance Statement is specifically for providers participating in the Minnesota Health Care Programs.
Form Details:
- Released on August 1, 2021;
- The latest edition provided by the Minnesota Department of Human Services;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form DHS-6189K-ENG by clicking the link below or browse more documents and templates provided by the Minnesota Department of Human Services.
Download Form DHS-6189K-ENG Homemaker Provider Assurance Statement - Minnesota Health Care Programs (Mhcp) - Minnesota
1
2
3