![]() This version of the form is not currently in use and is provided for reference only. Download this version of
Form SFN168
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
Form SFN168
for the current year.
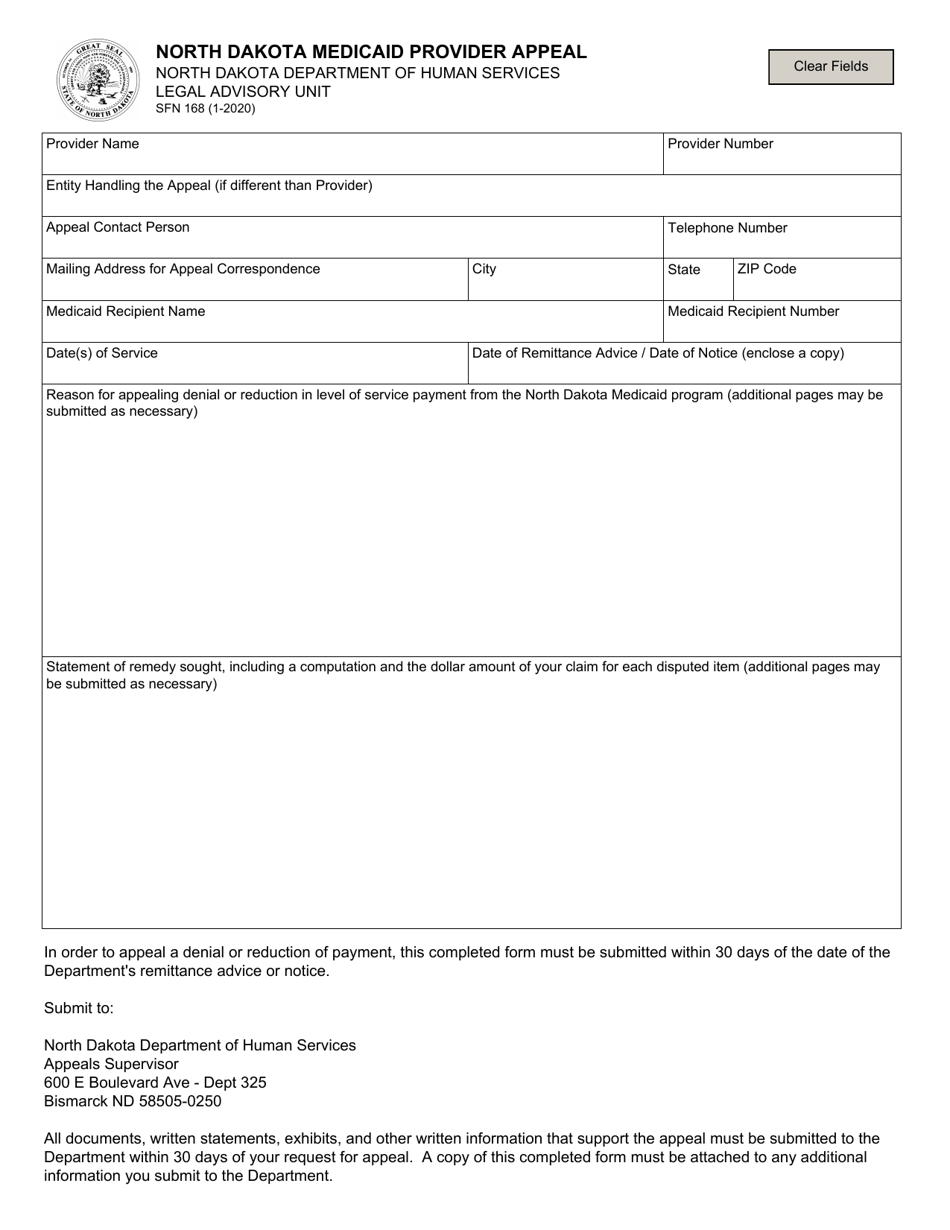
Form SFN168 North Dakota Medicaid Provider Appeal - North Dakota
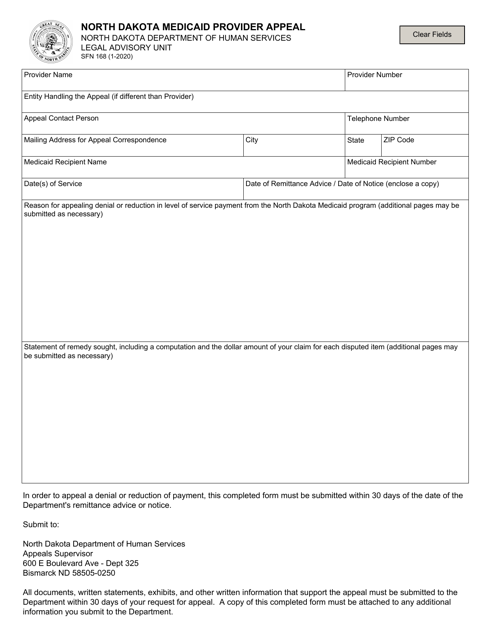
What Is Form SFN168?
This is a legal form that was released by the North Dakota Department of Health and Human Services - a government authority operating within North Dakota. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is Form SFN168?
A: Form SFN168 is a Medicaid Provider Appeal form used in North Dakota.
Q: What is the purpose of Form SFN168?
A: The purpose of Form SFN168 is to file an appeal for Medicaid reimbursement denials or other provider-related issues.
Q: Who can use Form SFN168?
A: Form SFN168 can be used by Medicaid providers in North Dakota.
Q: What information is required on Form SFN168?
A: Form SFN168 requires information such as provider details, statement of the issue, supporting documentation, and requested resolution.
Q: How do I submit Form SFN168?
A: Form SFN168 can be submitted by mail or fax to the North Dakota Department of Human Services.
Form Details:
- Released on January 1, 2020;
- The latest edition provided by the North Dakota Department of Health and Human Services;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form SFN168 by clicking the link below or browse more documents and templates provided by the North Dakota Department of Health and Human Services.