![]() This version of the form is not currently in use and is provided for reference only. Download this version of
the document
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
the document
for the current year.
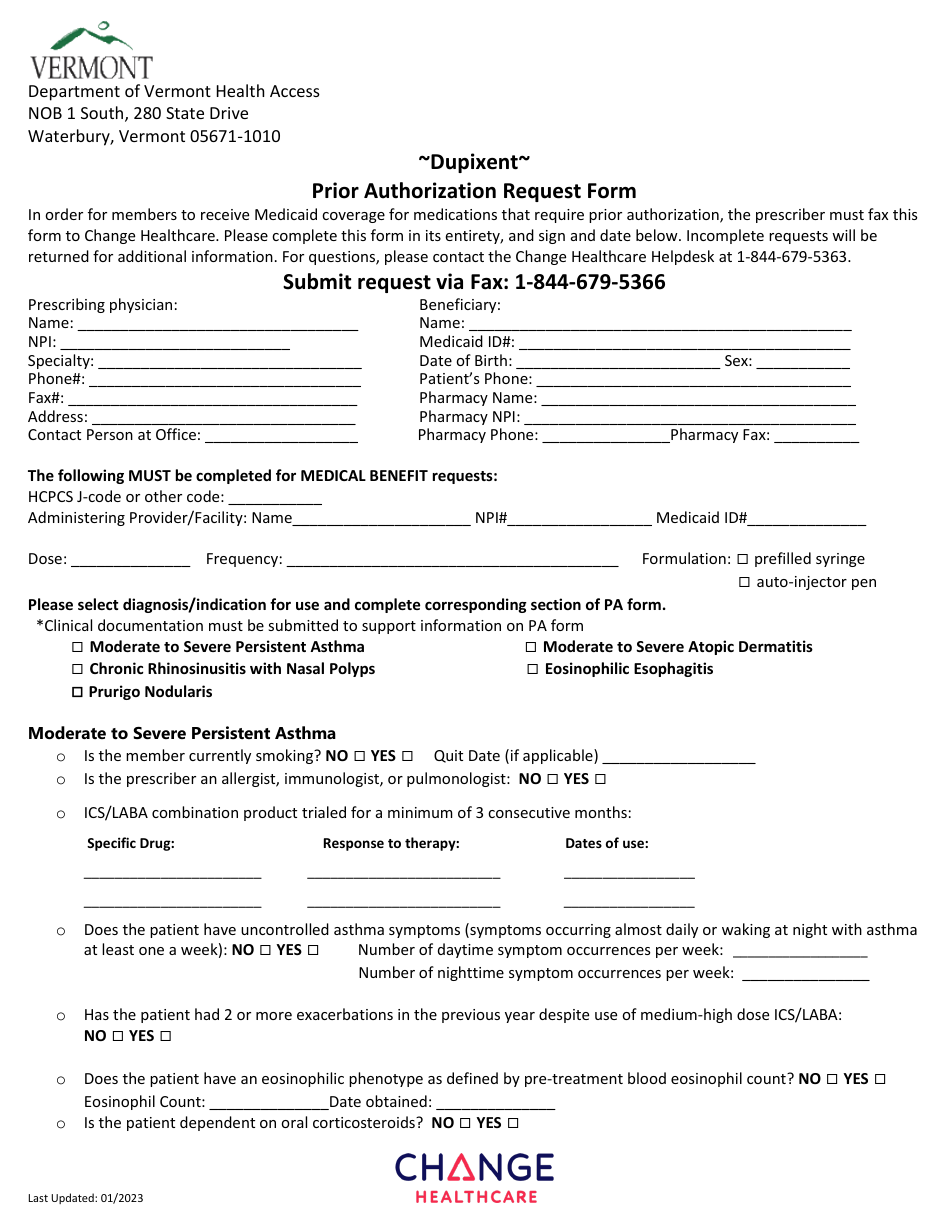
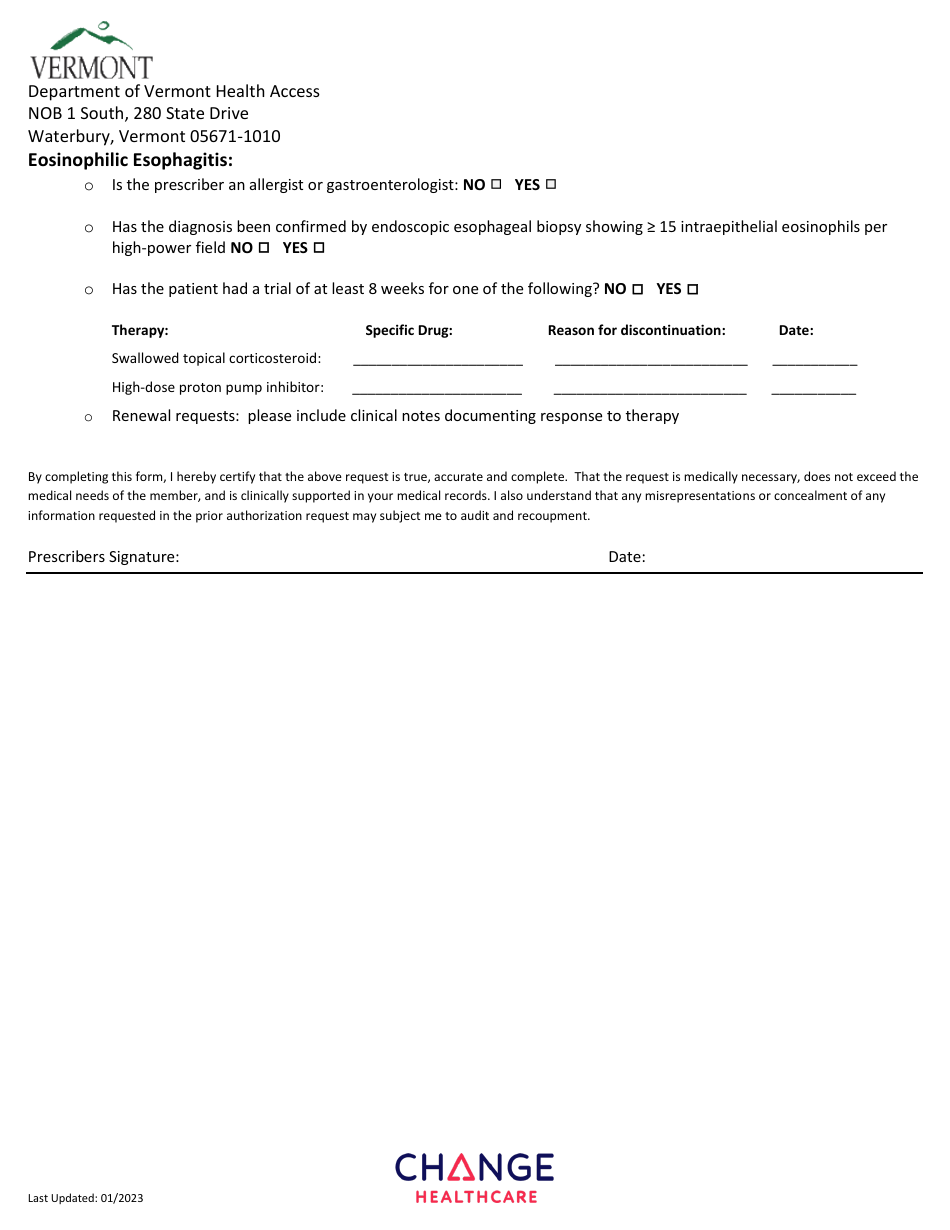
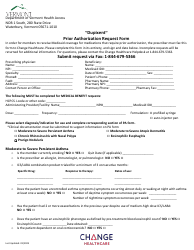
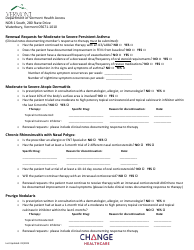
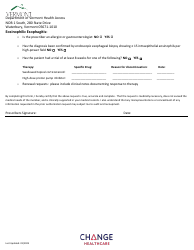
Dupixent Prior Authorization Request Form - Vermont
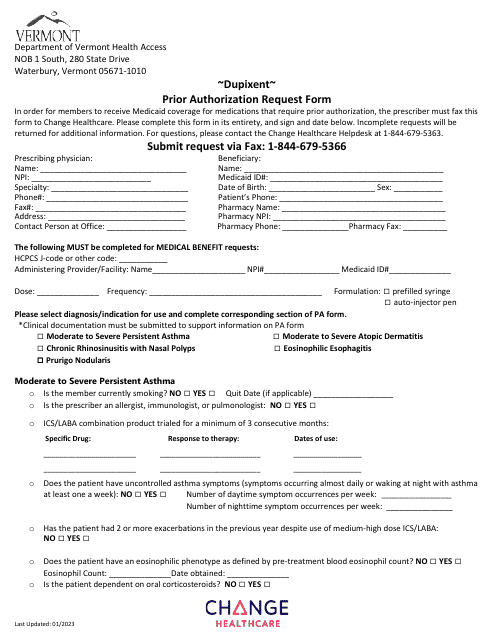
Dupixent Prior Authorization Request Form is a legal document that was released by the Department of Vermont Health Access - a government authority operating within Vermont.
FAQ
Q: What is the Dupixent Prior Authorization Request Form?
A: The Dupixent Prior Authorization Request Form is a form that needs to be filled out by your healthcare provider to request coverage for Dupixent, a medication for certain conditions.
Q: Why is a prior authorization required for Dupixent?
A: A prior authorization is required for Dupixent to ensure that the use of this medication is medically necessary and meets the criteria set by your insurance provider.
Q: What information is needed on the Dupixent Prior Authorization Request Form?
A: The form will typically require information such as your personal details, medical history, diagnosis, supporting documentation, and prescribing healthcare provider information.
Q: How long does it usually take for a Dupixent prior authorization to be approved?
A: The time for approval can vary, but it typically takes a few business days to a couple of weeks for a Dupixent prior authorization to be approved.
Q: What happens if the Dupixent prior authorization is denied?
A: If the prior authorization is denied, you can usually appeal the decision or discuss alternative options with your healthcare provider and insurance provider.
Q: Does a Dupixent prior authorization guarantee coverage?
A: No, a prior authorization does not guarantee coverage, but it helps determine whether your insurance provider will cover the cost of Dupixent.
Q: Can I get assistance with filling out the Dupixent Prior Authorization Request Form?
A: Yes, your healthcare provider's office or your insurance provider may be able to provide guidance and assistance with filling out the form.
Q: Is the Dupixent Prior Authorization Request Form specific to Vermont?
A: Yes, the Dupixent Prior Authorization Request Form you have mentioned is specific to Vermont. Other states may have their own forms or requirements.
Form Details:
- Released on January 1, 2023;
- The latest edition currently provided by the Department of Vermont Health Access;
- Ready to use and print;
- Easy to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a printable version of the form by clicking the link below or browse more documents and templates provided by the Department of Vermont Health Access.
Download Dupixent Prior Authorization Request Form - Vermont
1
2
3