![]() This version of the form is not currently in use and is provided for reference only. Download this version of
the document
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
the document
for the current year.
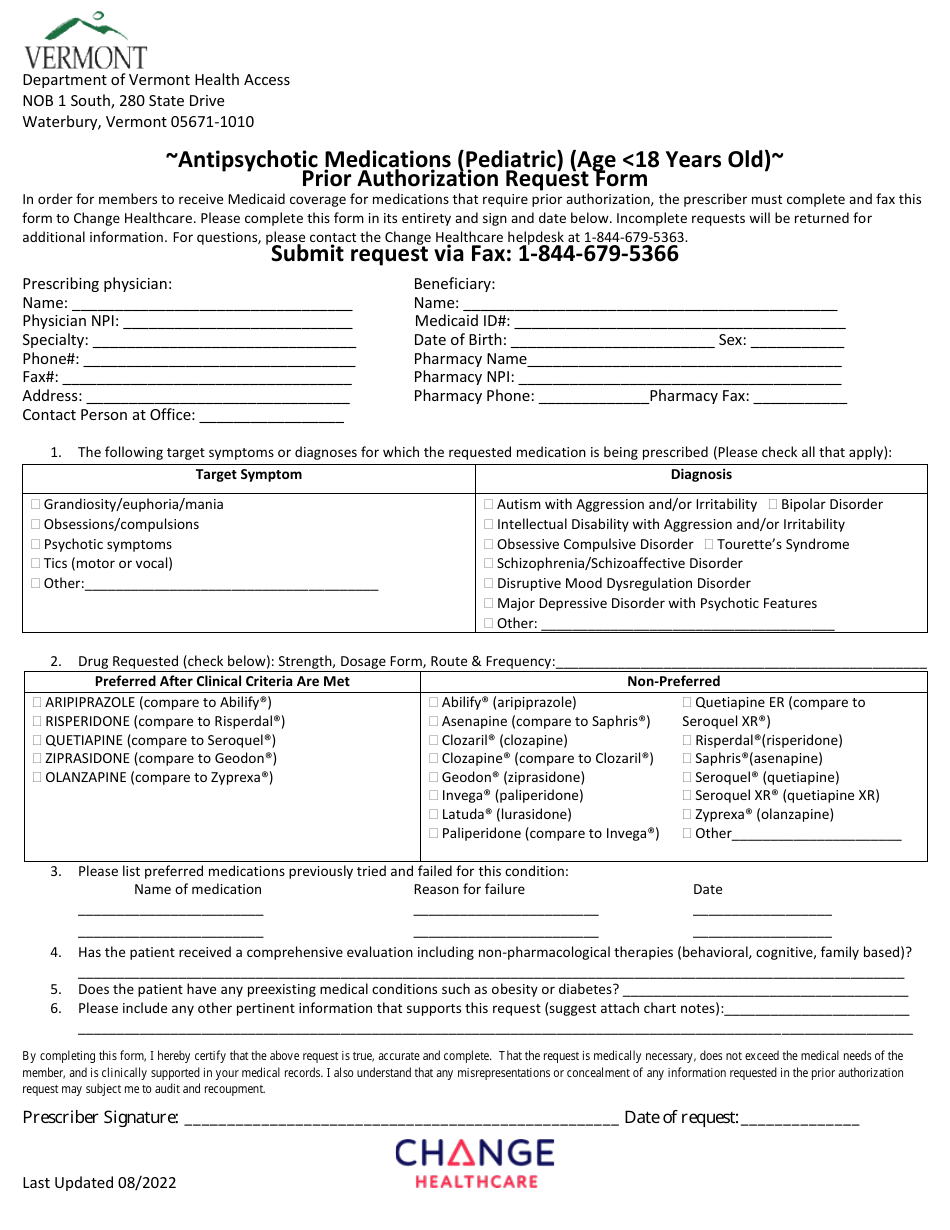
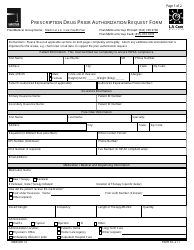
Antipsychotic Medications (Pediatric) (Age 18 Years Old) Prior Authorization Request Form - Vermont
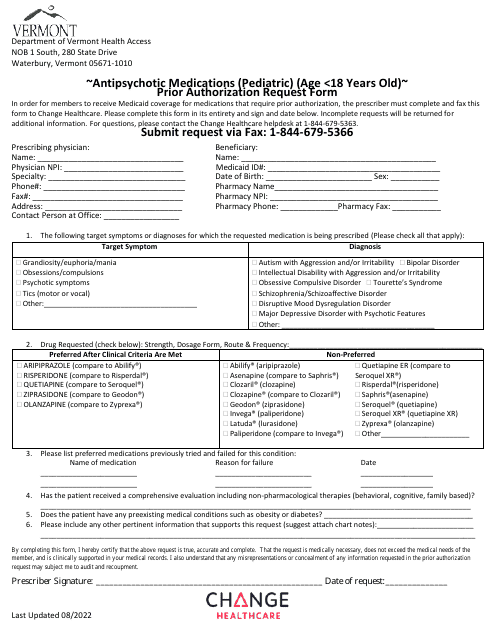
Antipsychotic Medications (Pediatric) (Age 18 Years Old) Prior Authorization Request Form is a legal document that was released by the Department of Vermont Health Access - a government authority operating within Vermont.
FAQ
Q: What is the purpose of the Antipsychotic Medications Prior Authorization Request Form?
A: The form is used to request prior authorization for antipsychotic medications in pediatrics (up to 18 years old) in Vermont.
Q: What age group does the Antipsychotic Medications Prior Authorization Request Form apply to?
A: The form applies to pediatric patients up to 18 years old.
Q: What is the purpose of prior authorization for antipsychotic medications?
A: Prior authorization ensures that the use of antipsychotic medications is appropriate and necessary for the patient.
Q: Who can use the Antipsychotic Medications Prior Authorization Request Form?
A: Healthcare providers who are prescribing antipsychotic medications for pediatric patients up to 18 years old in Vermont can use the form.
Form Details:
- Released on August 1, 2022;
- The latest edition currently provided by the Department of Vermont Health Access;
- Ready to use and print;
- Easy to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a printable version of the form by clicking the link below or browse more documents and templates provided by the Department of Vermont Health Access.