![]() This version of the form is not currently in use and is provided for reference only. Download this version of
Form HCA20-0167
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
Form HCA20-0167
for the current year.
Form HCA20-0167 Sebb Continuation Coverage Notice of Appeal - Washington
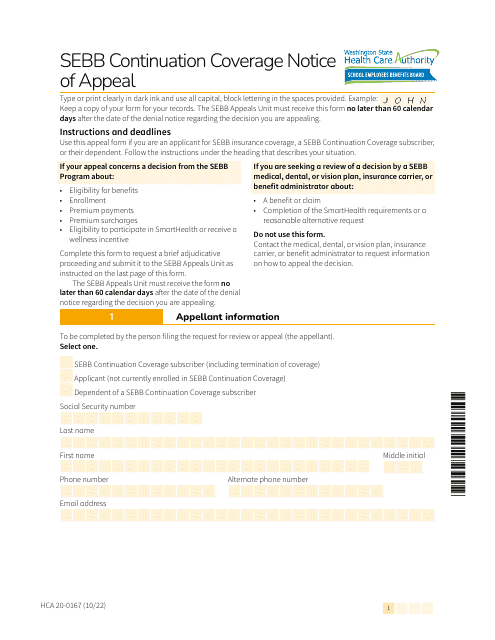
What Is Form HCA20-0167?
This is a legal form that was released by the Washington State Health Care Authority - a government authority operating within Washington. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is Form HCA20-0167?
A: Form HCA20-0167 is the Sebb Continuation Coverage Notice of Appeal form specifically for residents of Washington.
Q: What is Sebb Continuation Coverage?
A: Sebb Continuation Coverage is a program that allows eligible individuals to continue their health insurance coverage after certain qualifying events.
Q: Who can file Form HCA20-0167?
A: Form HCA20-0167 can be filed by individuals who wish to appeal a decision related to their Sebb Continuation Coverage in Washington.
Q: What is the purpose of the Notice of Appeal?
A: The purpose of the Notice of Appeal is to request a review of a decision regarding Sebb Continuation Coverage.
Q: What information is required on Form HCA20-0167?
A: Form HCA20-0167 requires information such as the appellant's name, contact information, a description of the decision being appealed, and any supporting documentation.
Form Details:
- Released on October 1, 2022;
- The latest edition provided by the Washington State Health Care Authority;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form HCA20-0167 by clicking the link below or browse more documents and templates provided by the Washington State Health Care Authority.
Download Form HCA20-0167 Sebb Continuation Coverage Notice of Appeal - Washington

1
2

3

4