Form F-01423 Insurance Enrollment Report - AIDS / HIV Drug Assistance and Insurance Assistance Program - Wisconsin
What Is Form F-01423?
This is a legal form that was released by the Wisconsin Department of Health Services - a government authority operating within Wisconsin. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is Form F-01423?
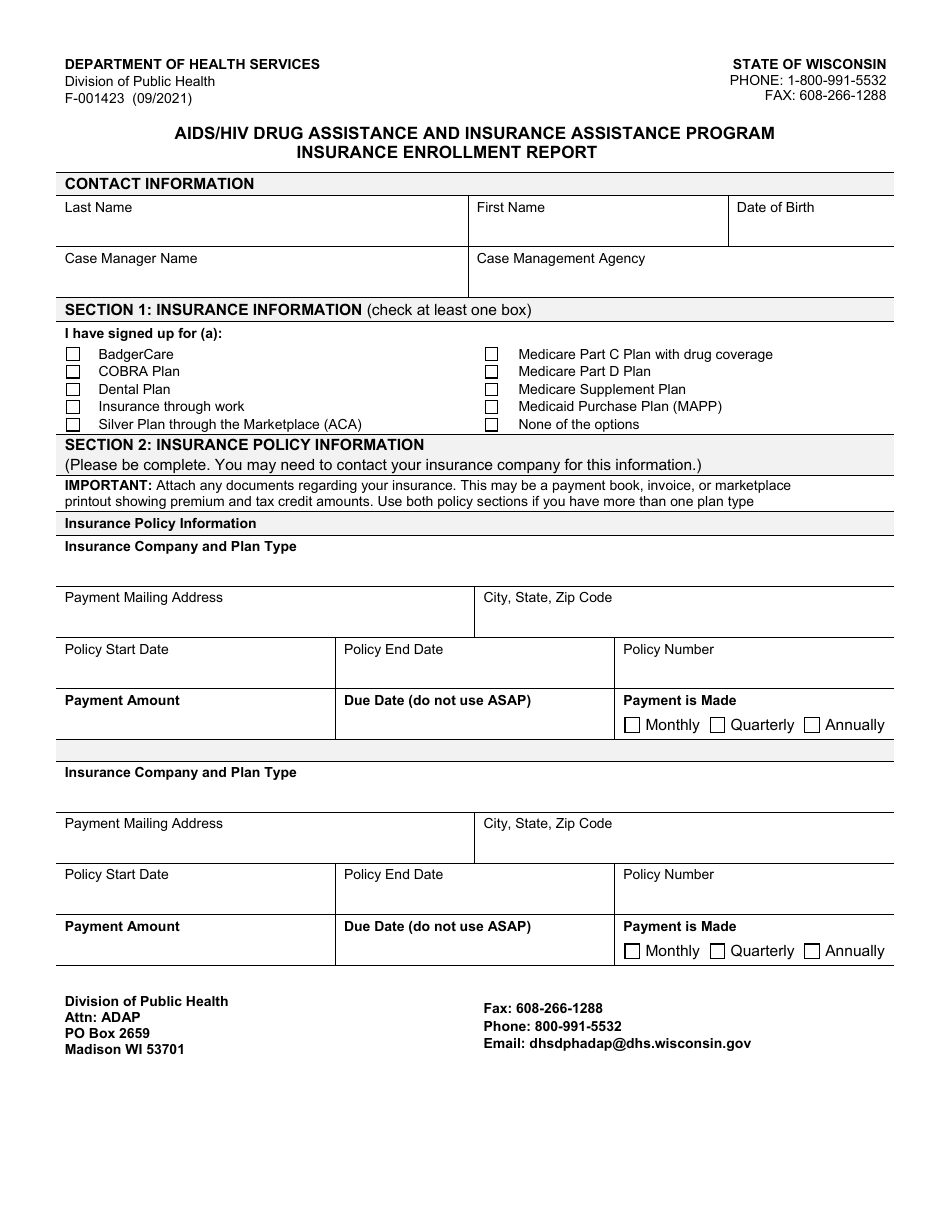
A: Form F-01423 is the Insurance Enrollment Report for the AIDS/HIV Drug Assistance and Insurance Assistance Program in Wisconsin.
Q: What is the purpose of Form F-01423?
A: The purpose of Form F-01423 is to provide enrollment information for the AIDS/HIV Drug Assistance and Insurance Assistance Program in Wisconsin.
Q: Who is required to complete Form F-01423?
A: Healthcare providers and insurers are required to complete Form F-01423.
Q: What information is included in Form F-01423?
A: Form F-01423 includes information about the applicant's insurance coverage, medication usage, and other relevant details.
Q: Are there any fees associated with Form F-01423?
A: There are no fees associated with completing and submitting Form F-01423.
Q: Who should I contact for questions about Form F-01423?
A: For questions about Form F-01423, you should contact the Wisconsin Department of Health Services or your healthcare provider.
Form Details:
- Released on September 1, 2021;
- The latest edition provided by the Wisconsin Department of Health Services;
- Easy to use and ready to print;
- Available in Spanish;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form F-01423 by clicking the link below or browse more documents and templates provided by the Wisconsin Department of Health Services.