Form F-01161 Abortion Certification Statements - Wisconsin
What Is Form F-01161?
This is a legal form that was released by the Wisconsin Department of Health Services - a government authority operating within Wisconsin. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is Form F-01161?
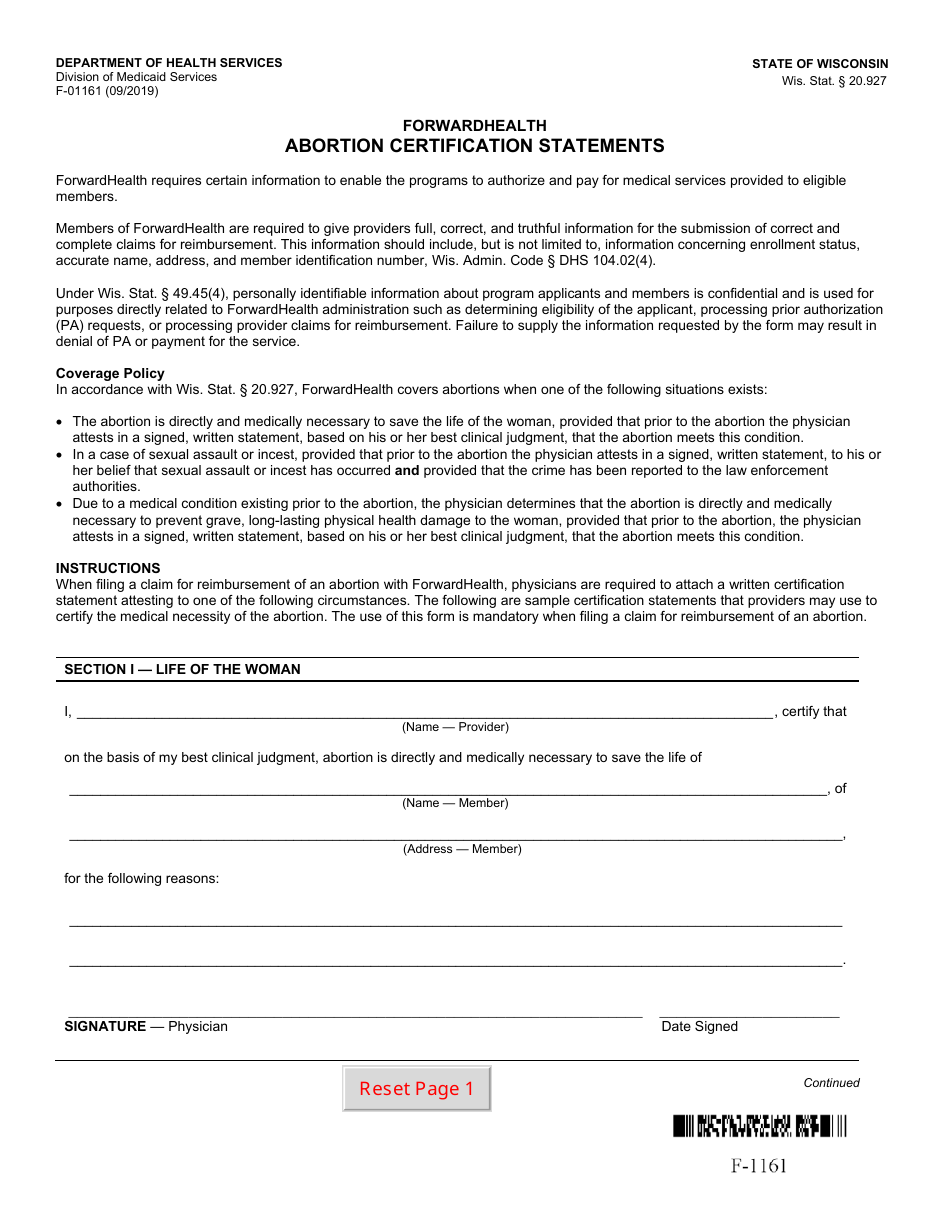
A: Form F-01161 is the Abortion Certification Statements form used in the state of Wisconsin.
Q: Who uses Form F-01161?
A: Form F-01161 is used by physicians and facilities performing abortions in Wisconsin.
Q: What is the purpose of Form F-01161?
A: The purpose of Form F-01161 is to certify that specific requirements have been met for an abortion procedure.
Q: What information is included in Form F-01161?
A: Form F-01161 includes information such as the patient's name, gestational age, and the physician's certification.
Q: Do I need to submit Form F-01161 to the state?
A: Yes, Form F-01161 must be submitted to the state within 30 days of the abortion procedure.
Q: Who is responsible for completing Form F-01161?
A: The physician who performs the abortion procedure is responsible for completing Form F-01161.
Q: Are there any penalties for not submitting Form F-01161?
A: Failure to submit Form F-01161 can result in penalties and the suspension of a physician's license.
Q: What if I have further questions about Form F-01161?
A: If you have further questions about Form F-01161, you can contact the Wisconsin Department of Health Services for assistance.
Form Details:
- Released on September 1, 2019;
- The latest edition provided by the Wisconsin Department of Health Services;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form F-01161 by clicking the link below or browse more documents and templates provided by the Wisconsin Department of Health Services.
Download Form F-01161 Abortion Certification Statements - Wisconsin
1
2