Form F-01188 Wisconsin Adult Cystic Fibrosis Program - Financial Need Statement - Wisconsin
What Is Form F-01188?
This is a legal form that was released by the Wisconsin Department of Health Services - a government authority operating within Wisconsin. Check the official instructions before completing and submitting the form.
FAQ
Q: What is Form F-01188?
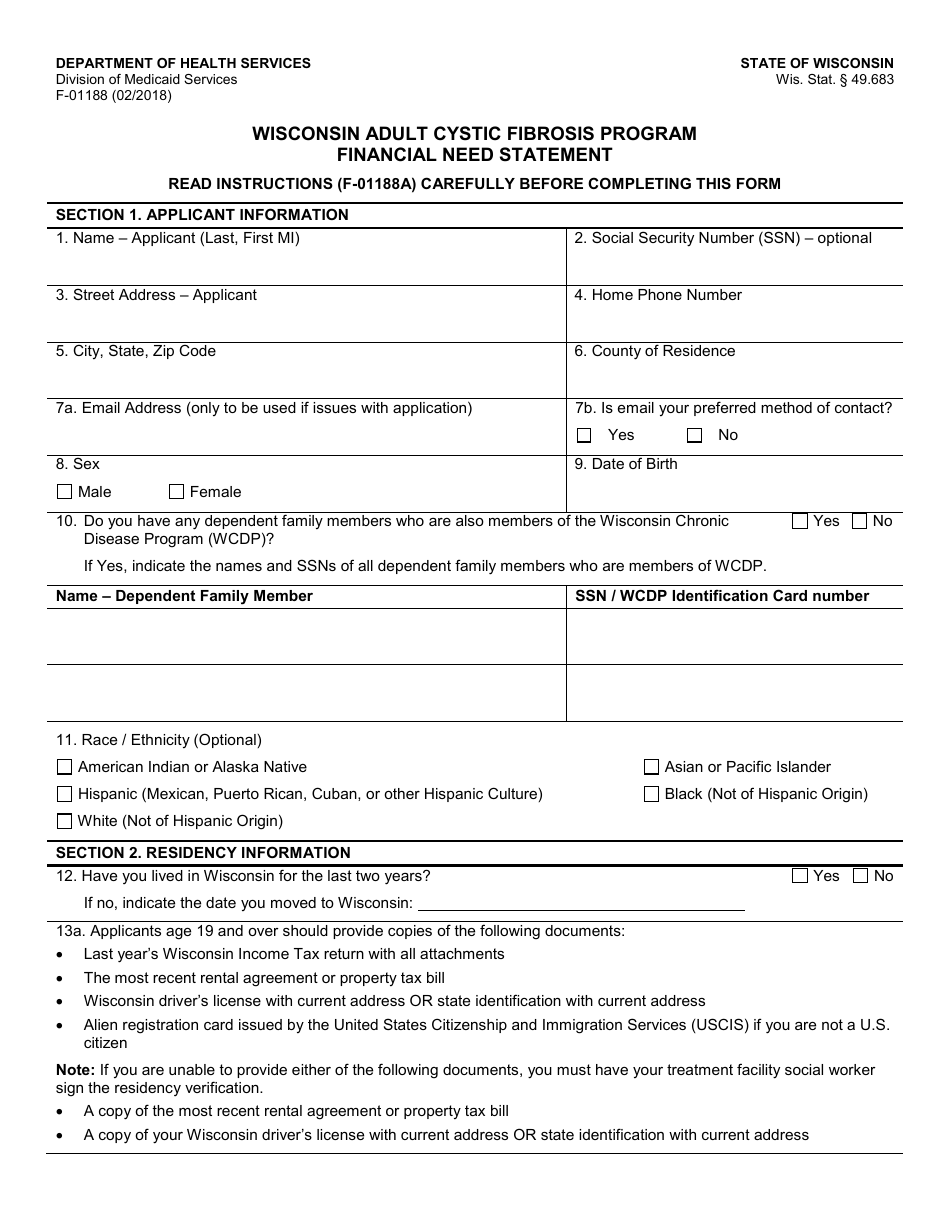
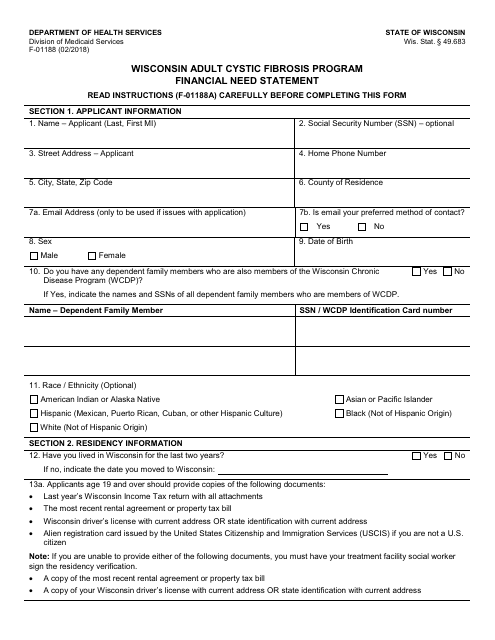
A: Form F-01188 is the Wisconsin Adult Cystic Fibrosis Program - Financial Need Statement form.
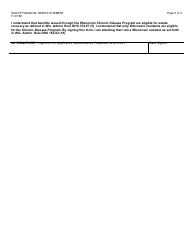
Q: Who is eligible for the Wisconsin Adult Cystic Fibrosis Program?
A: Adults with cystic fibrosis who meet the program's eligibility criteria are eligible for the Wisconsin Adult Cystic Fibrosis Program.
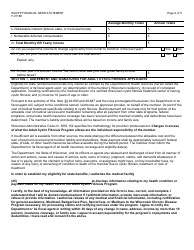
Q: What is the purpose of the Financial Need Statement?
A: The Financial Need Statement is used to assess the financial need of individuals applying for the Wisconsin Adult Cystic Fibrosis Program.
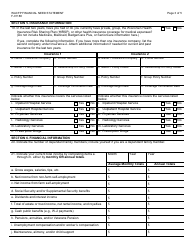
Q: What information is required in the Financial Need Statement?
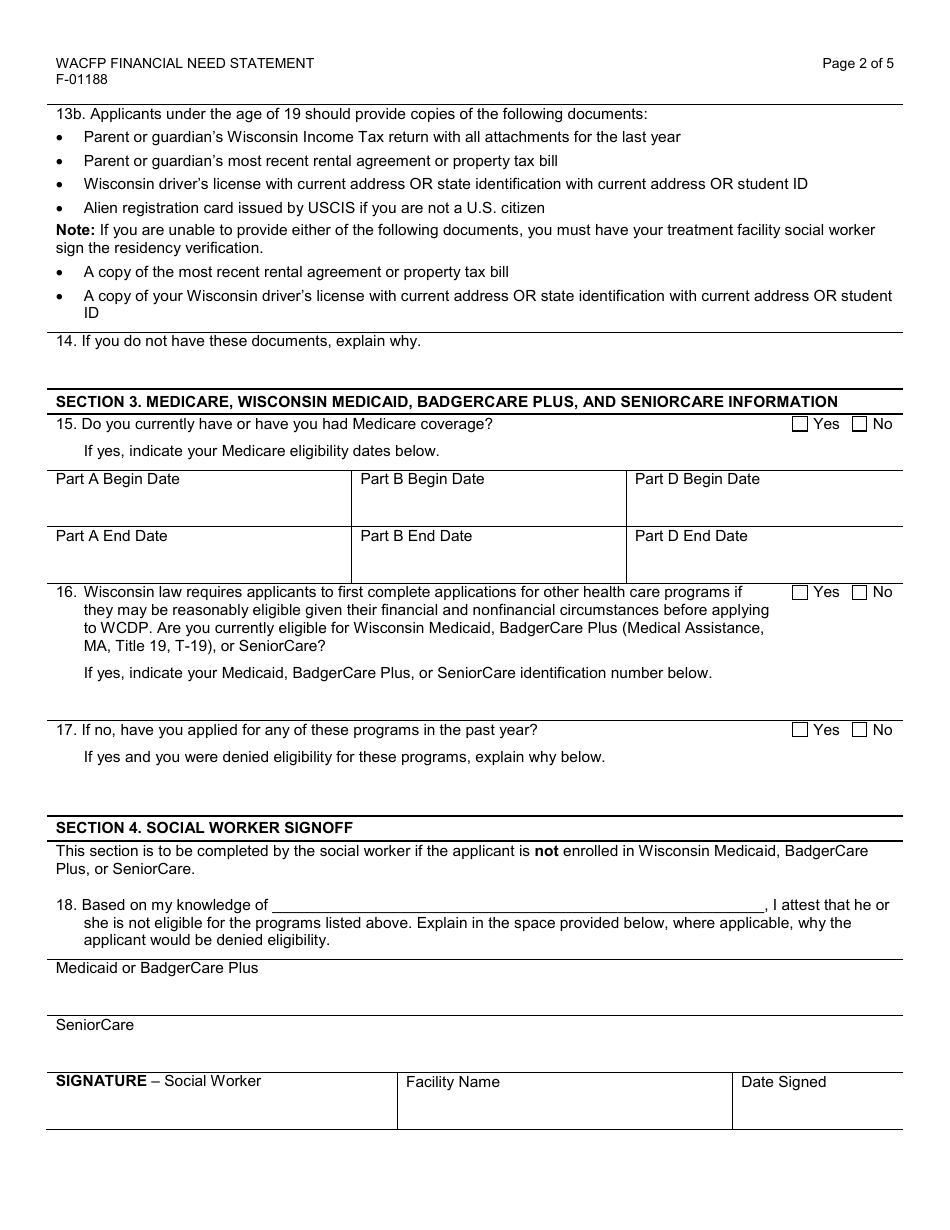
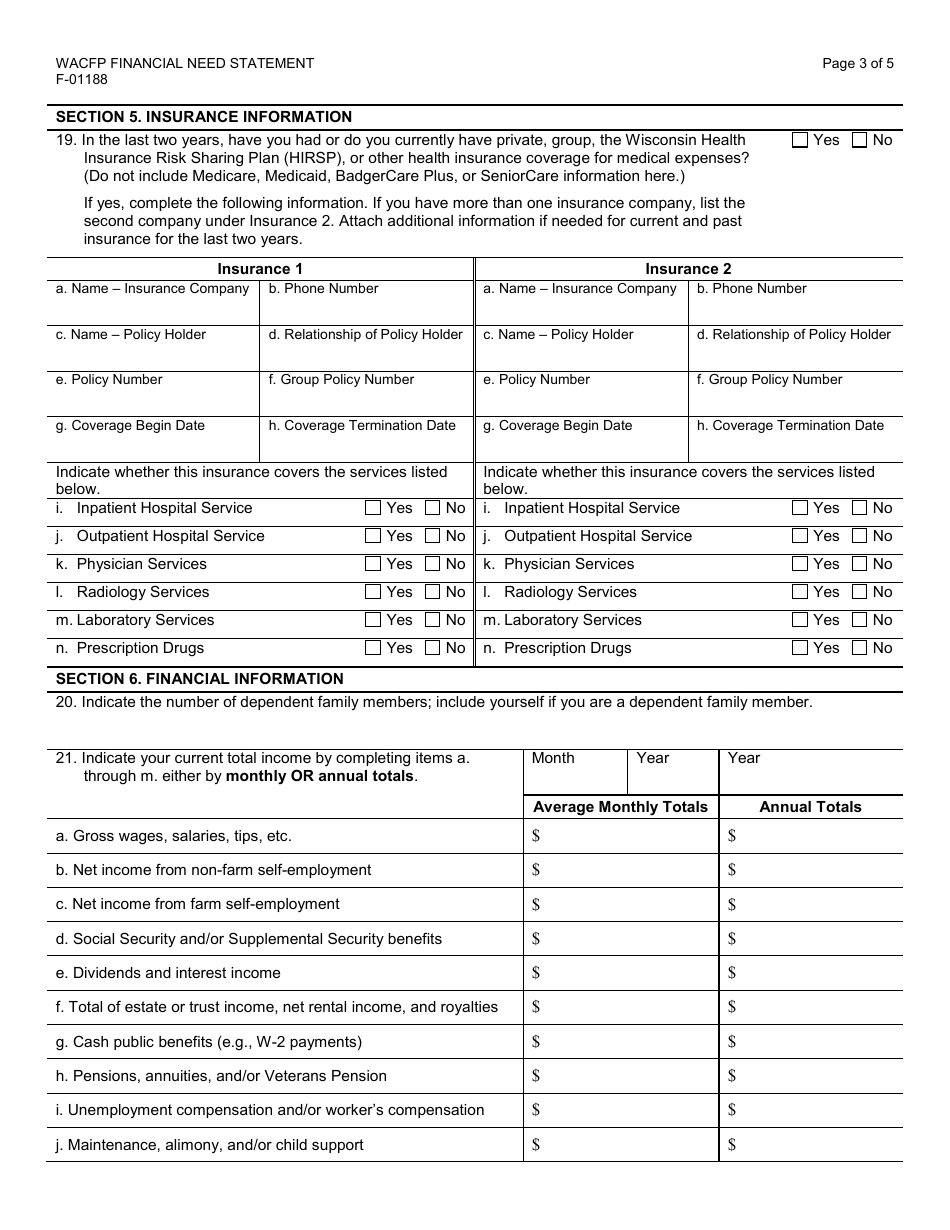
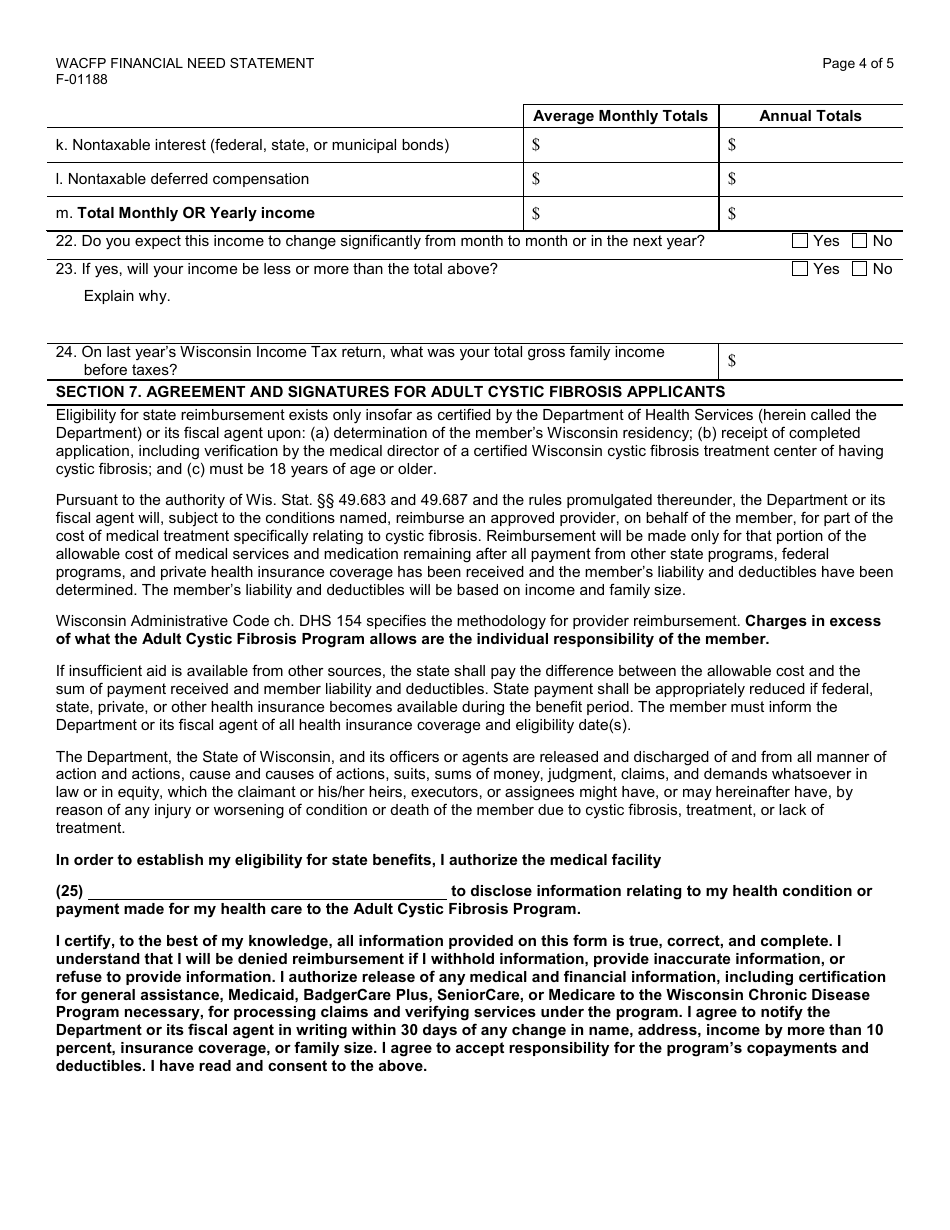
A: The Financial Need Statement requires information on income, assets, expenses, and other financial details.
Q: Can I apply for the program without submitting the Financial Need Statement?
A: No, the Financial Need Statement is a required part of the application process for the Wisconsin Adult Cystic Fibrosis Program.
Q: What happens after I submit the Financial Need Statement?
A: After you submit the Financial Need Statement, it will be reviewed by the Wisconsin Adult Cystic Fibrosis Program to determine your eligibility for financial assistance.
Q: Is the Wisconsin Adult Cystic Fibrosis Program limited to residents of Wisconsin?
A: Yes, the Wisconsin Adult Cystic Fibrosis Program is available only to residents of Wisconsin.
Form Details:
- Released on February 1, 2018;
- The latest edition provided by the Wisconsin Department of Health Services;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a printable version of Form F-01188 by clicking the link below or browse more documents and templates provided by the Wisconsin Department of Health Services.
Download Form F-01188 Wisconsin Adult Cystic Fibrosis Program - Financial Need Statement - Wisconsin
1
2
3
4
5