Form F-00433 Prior Authorization / Preferred Drug List (Pa / Pdl) for Proton Pump Inhibitor (Ppi) Orally Disintegrating Tablets - Wisconsin
What Is Form F-00433?
This is a legal form that was released by the Wisconsin Department of Health Services - a government authority operating within Wisconsin. Check the official instructions before completing and submitting the form.
FAQ
Q: What is Form F-00433?
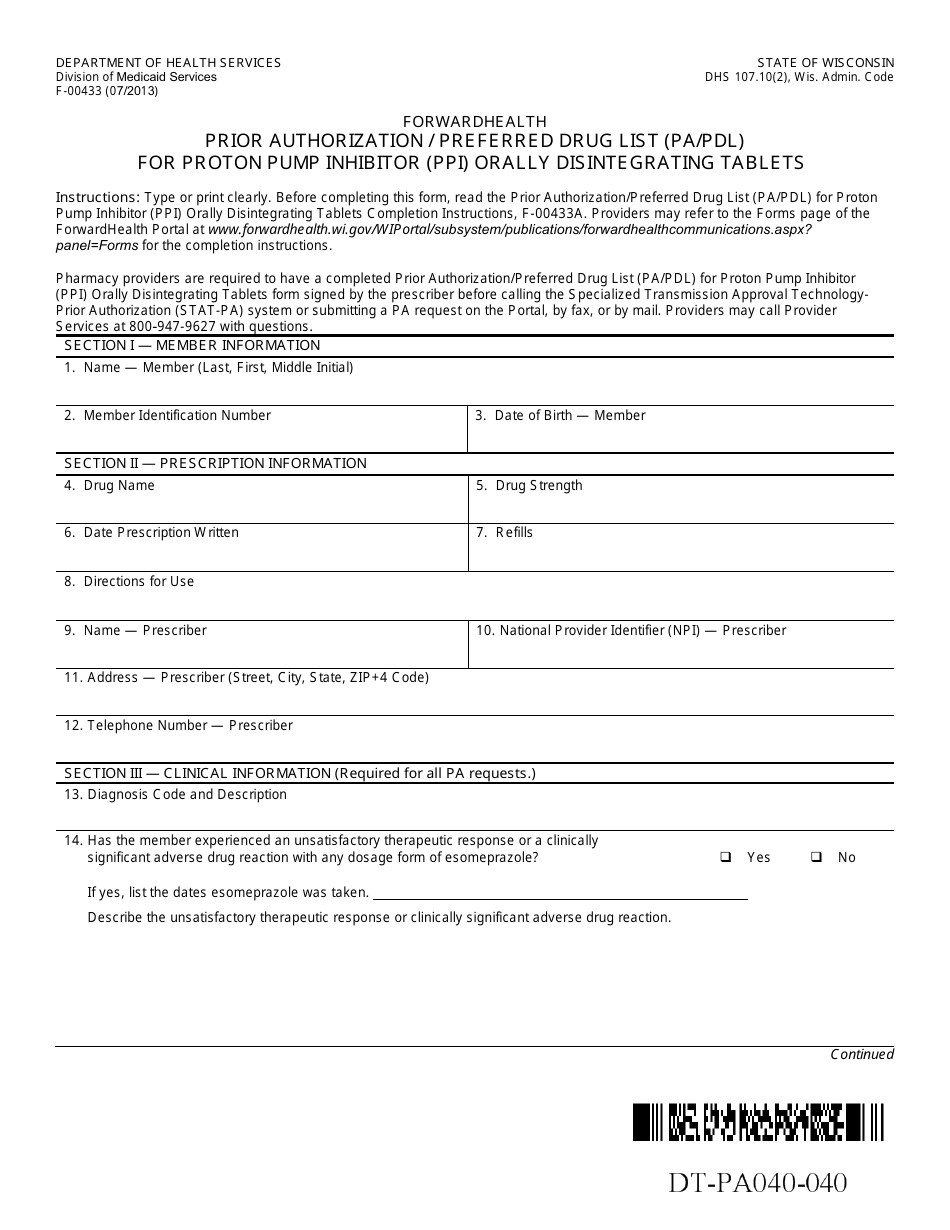
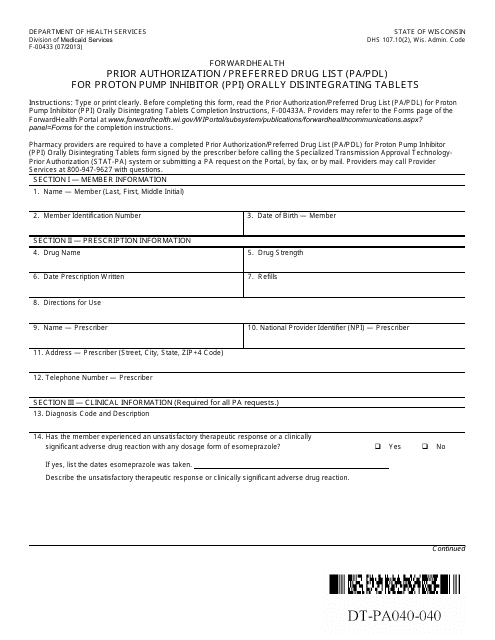
A: Form F-00433 is the Prior Authorization/Preferred Drug List for Proton Pump Inhibitor (PPI) Orally Disintegrating Tablets in Wisconsin.
Q: What is a Prior Authorization/Preferred Drug List (PA/PDL)?
A: A Prior Authorization/Preferred Drug List (PA/PDL) is a form or list used by healthcare providers and insurance companies to determine coverage and approval for certain medications.
Q: What are Proton Pump Inhibitors (PPIs)?
A: Proton Pump Inhibitors (PPIs) are a type of medication used to reduce the amount of acid produced by the stomach. They are commonly prescribed for conditions such as acid reflux and ulcers.
Q: What are Orally Disintegrating Tablets?
A: Orally Disintegrating Tablets are a type of medication that dissolves in the mouth without the need for water. They are often used for people who have difficulty swallowing pills.
Q: Why is prior authorization required for PPI Orally Disintegrating Tablets in Wisconsin?
A: Prior authorization may be required for PPI Orally Disintegrating Tablets in Wisconsin to ensure appropriate and cost-effective use of these medications.
Q: What is the purpose of the Preferred Drug List (PDL)?
A: The Preferred Drug List (PDL) is a list of medications preferred by an insurance company or pharmacy benefit manager, which may offer lower copayments or cost-sharing for these medications.
Q: How can I find out if a specific PPI Orally Disintegrating Tablet is covered by my insurance?
A: You can check with your insurance provider or consult the Prior Authorization/Preferred Drug List (PA/PDL) to find out if a specific PPI Orally Disintegrating Tablet is covered.
Q: Can my healthcare provider request prior authorization for a PPI Orally Disintegrating Tablet?
A: Yes, your healthcare provider can request prior authorization for a PPI Orally Disintegrating Tablet if it is medically necessary for your condition.
Form Details:
- Released on July 1, 2013;
- The latest edition provided by the Wisconsin Department of Health Services;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form F-00433 by clicking the link below or browse more documents and templates provided by the Wisconsin Department of Health Services.
Download Form F-00433 Prior Authorization / Preferred Drug List (Pa / Pdl) for Proton Pump Inhibitor (Ppi) Orally Disintegrating Tablets - Wisconsin
1

2
3