Form ODM01958 Referral for Medicaid Continuing Eligibility Review - Ohio
What Is Form ODM01958?
This is a legal form that was released by the Ohio Department of Medicaid - a government authority operating within Ohio. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is Form ODM01958?
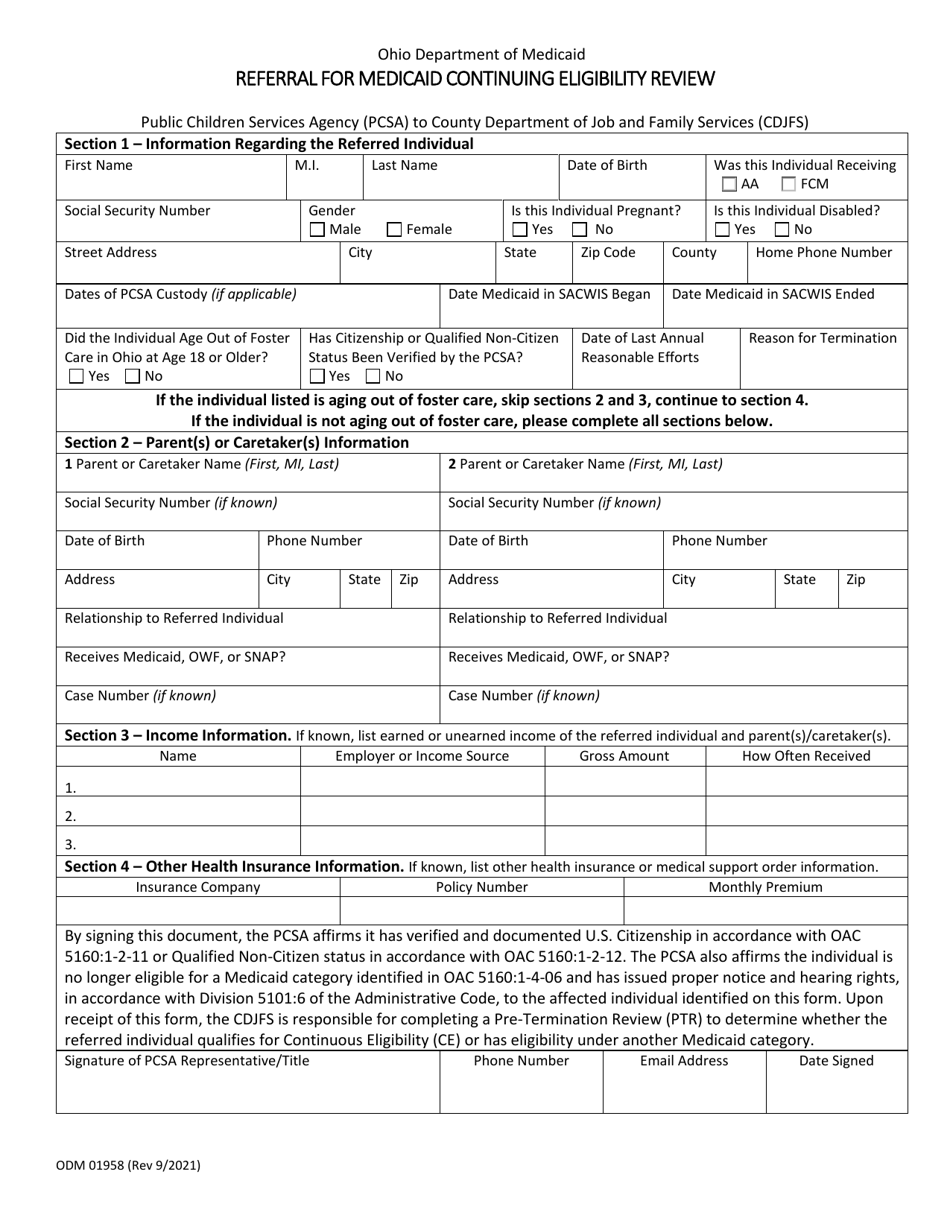
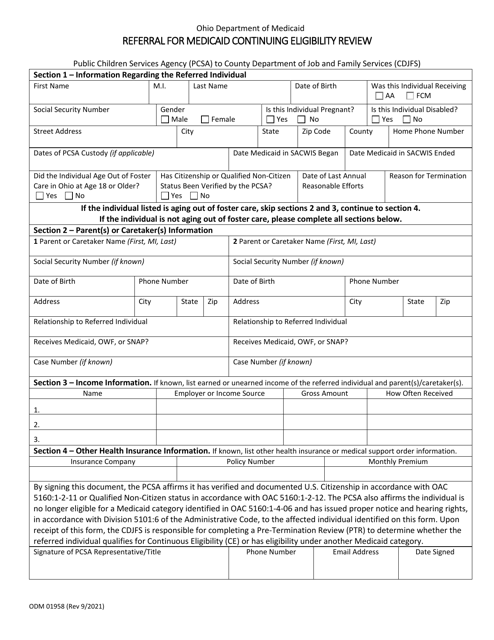
A: Form ODM01958 is a referral form for Medicaid continuing eligibility review in Ohio.
Q: Who needs to fill out Form ODM01958?
A: Form ODM01958 needs to be filled out by individuals who are currently receiving Medicaid benefits in Ohio and are required to undergo a continuing eligibility review.
Q: What is the purpose of Form ODM01958?
A: The purpose of Form ODM01958 is to refer individuals for a Medicaid continuing eligibility review in order to determine if they still meet the eligibility criteria for Medicaid benefits in Ohio.
Q: What information is required on Form ODM01958?
A: Form ODM01958 requires personal information, income details, employment status, and other relevant information to assess one's continuing eligibility for Medicaid benefits.
Q: How often do I need to fill out Form ODM01958?
A: The frequency of filling out Form ODM01958 for a Medicaid continuing eligibility review may vary based on individual circumstances. It is best to follow the instructions provided on the form or consult with the Ohio Department of Medicaid for specific guidance.
Form Details:
- Released on September 1, 2021;
- The latest edition provided by the Ohio Department of Medicaid;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form ODM01958 by clicking the link below or browse more documents and templates provided by the Ohio Department of Medicaid.