![]() This version of the form is not currently in use and is provided for reference only. Download this version of
Form HCA20-0167
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
Form HCA20-0167
for the current year.
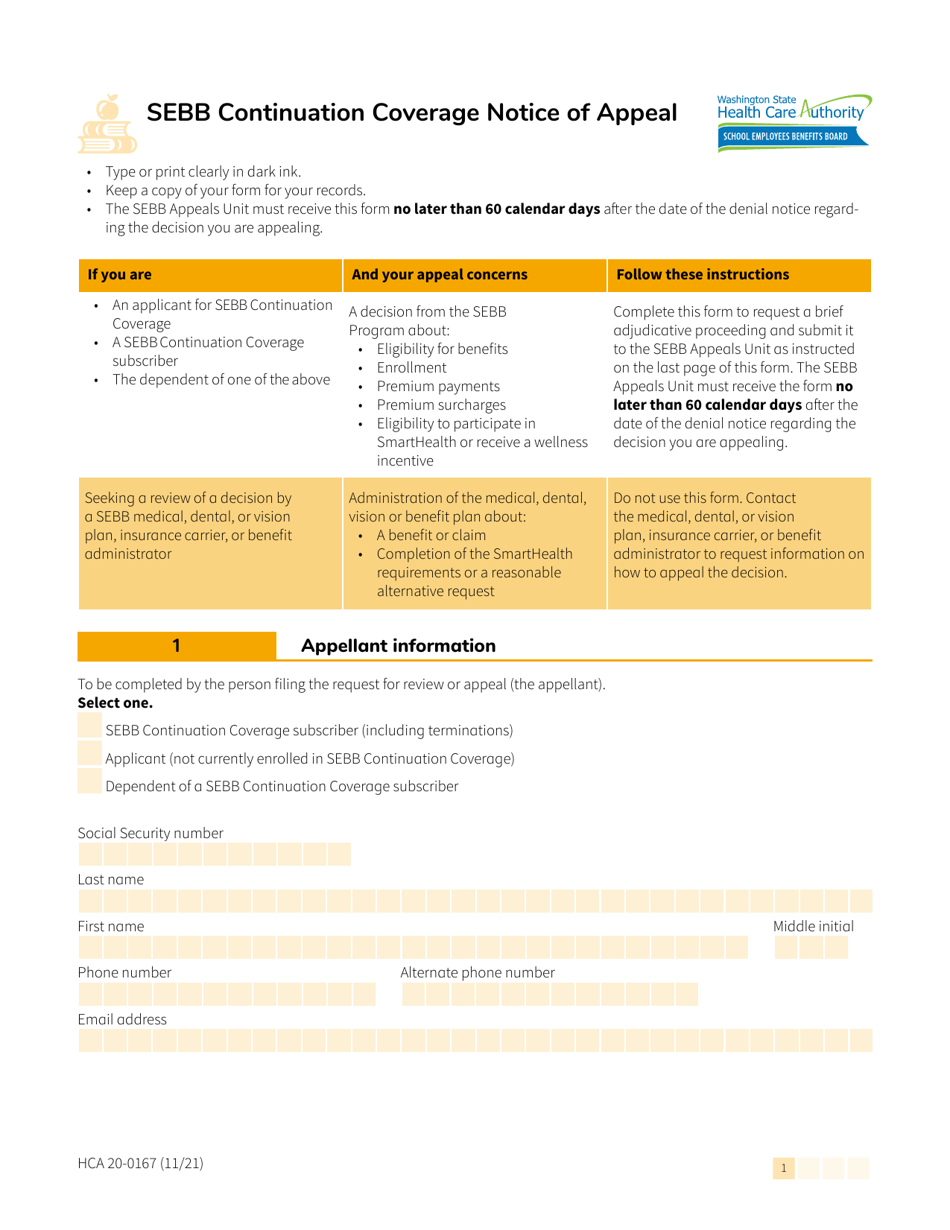
Form HCA20-0167 Sebb Continuation Coverage Notice of Appeal - Washington
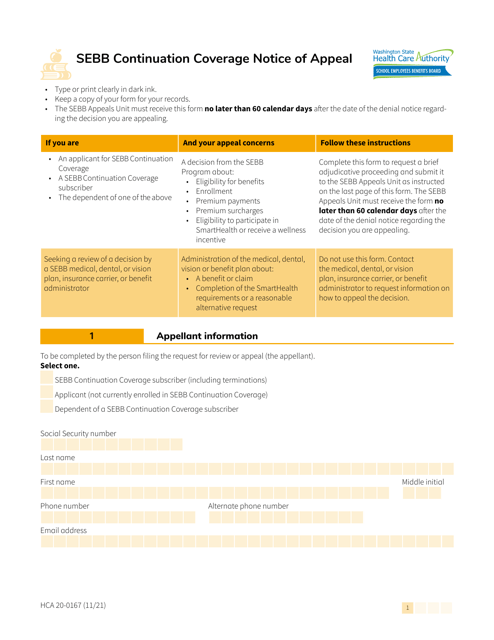
What Is Form HCA20-0167?
This is a legal form that was released by the Washington State Health Care Authority - a government authority operating within Washington. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is Form HCA20-0167?
A: Form HCA20-0167 is the Sebb Continuation Coverage Notice of Appeal form for Washington.
Q: Who is this form for?
A: This form is for individuals who want to appeal the denial of their Sebb Continuation Coverage in Washington.
Q: What is Sebb Continuation Coverage?
A: Sebb Continuation Coverage refers to the continuation of health coverage for eligible individuals who are no longer eligible for the State Employees Benefits Board (Sebb) program.
Q: Why would someone need to file an appeal?
A: Someone would need to file an appeal if their Sebb Continuation Coverage was denied and they believe it was done incorrectly.
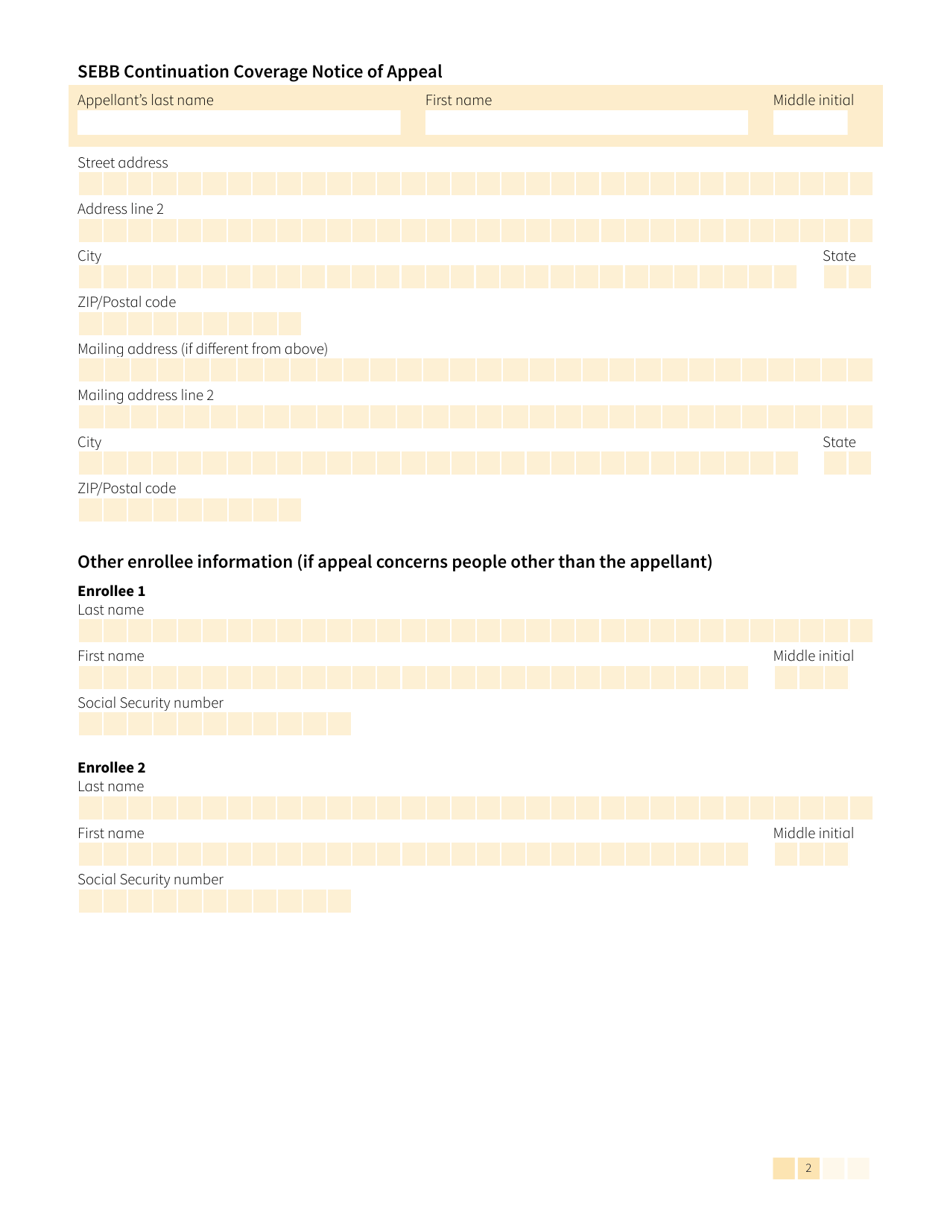
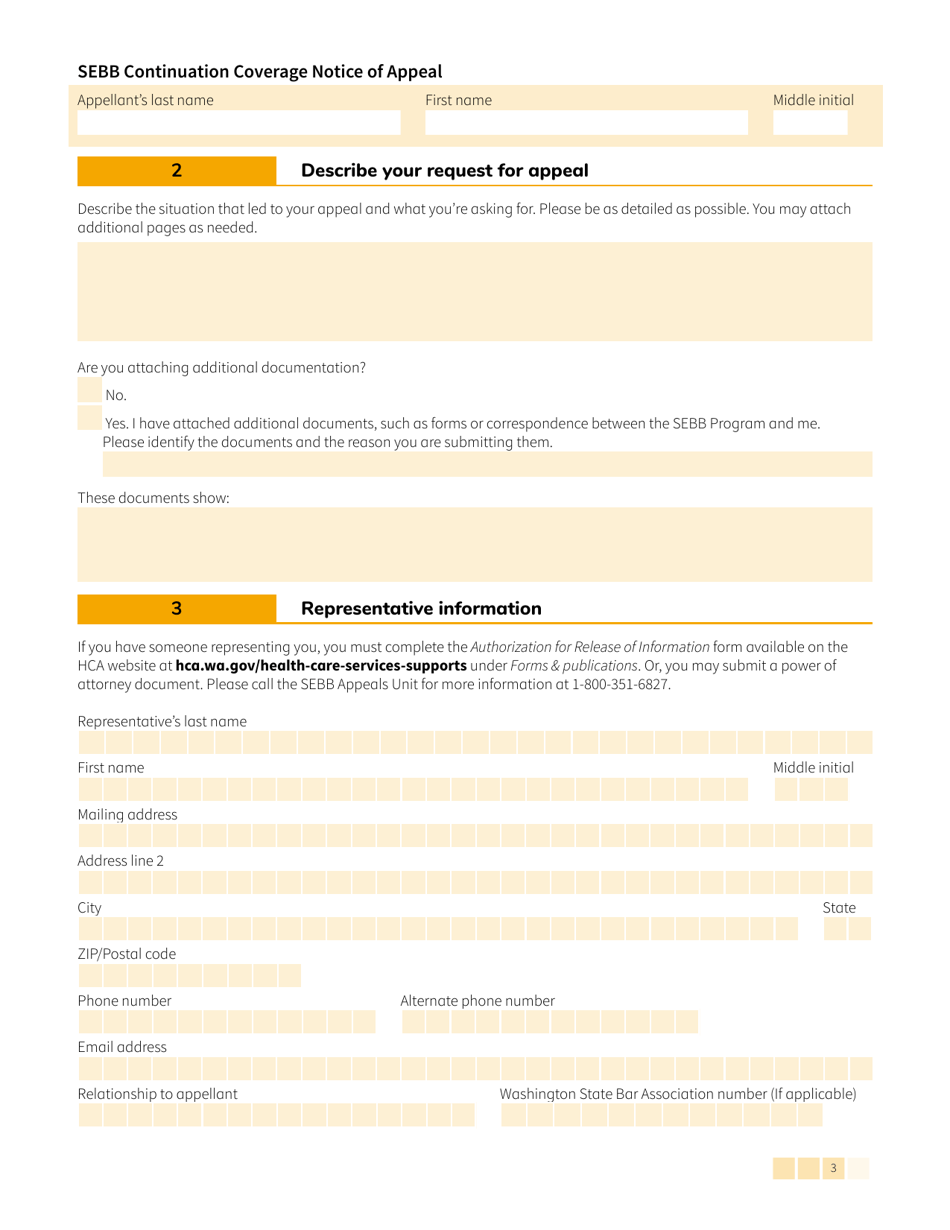
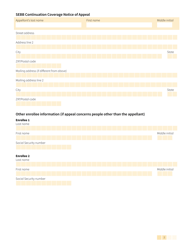
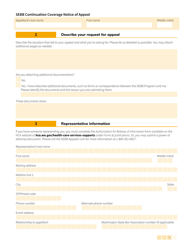
Q: What information do I need to provide on this form?
A: You need to provide your personal information, details about your denied Sebb Continuation Coverage, and the reasons why you are appealing.
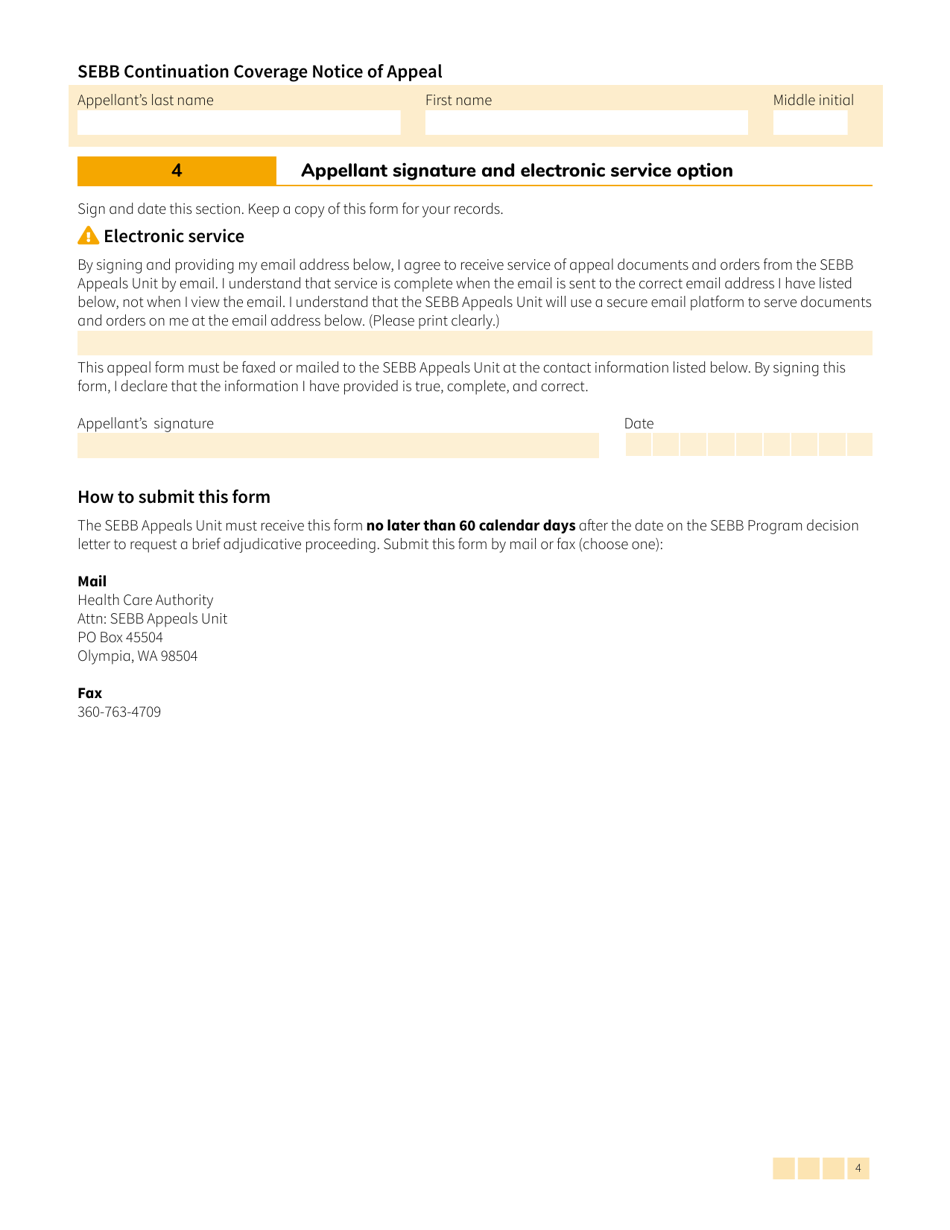
Q: What happens after I submit this form?
A: After you submit this form, the HCA will review your appeal and make a decision based on the information provided.
Q: Are there any deadlines for submitting this form?
A: Yes, there are deadlines for submitting this form. It is important to review the instructions and follow the specified timeframes.
Q: Can I get assistance in filling out this form?
A: Yes, you can seek assistance from the HCA or other authorized entities in filling out this form.
Q: Is there a fee for filing this appeal?
A: No, there is no fee for filing this appeal.
Form Details:
- Released on November 1, 2021;
- The latest edition provided by the Washington State Health Care Authority;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form HCA20-0167 by clicking the link below or browse more documents and templates provided by the Washington State Health Care Authority.
Download Form HCA20-0167 Sebb Continuation Coverage Notice of Appeal - Washington

1
2
3

4