Form F-02314 Wisconsin Tuberculosis (Tb) Risk Assessment and Symptom Evaluation - Wisconsin
What Is Form F-02314?
This is a legal form that was released by the Wisconsin Department of Health Services - a government authority operating within Wisconsin. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is Form F-02314?
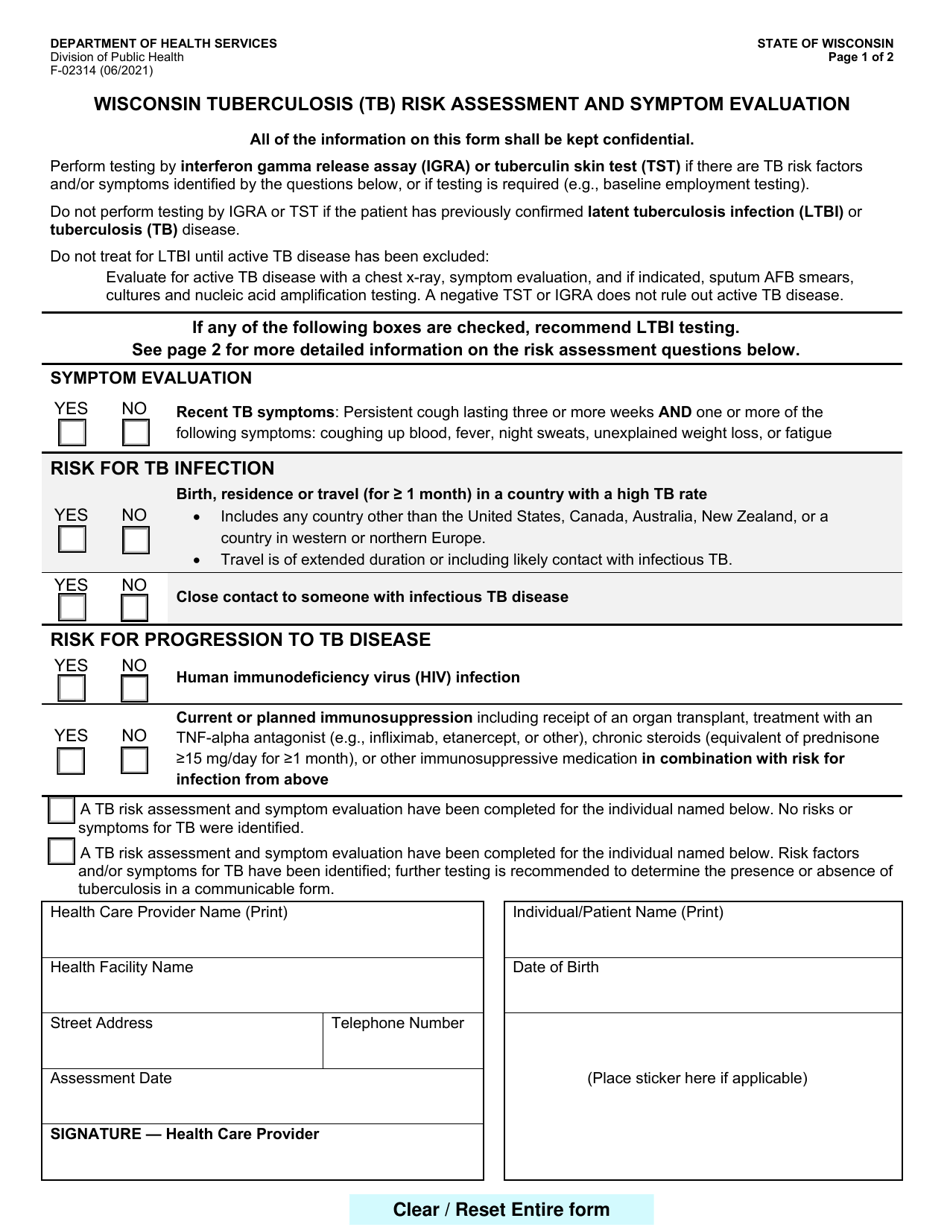
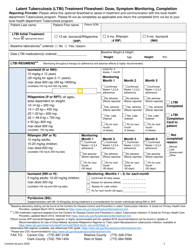
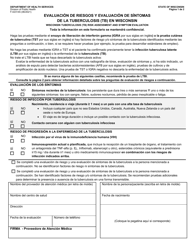
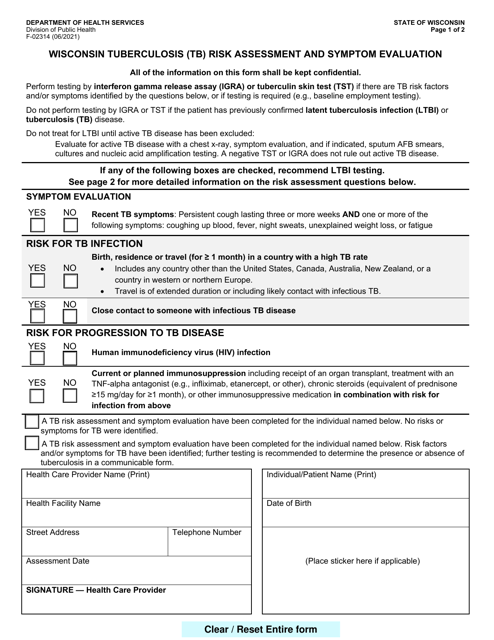
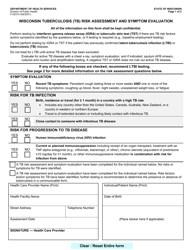
A: Form F-02314 is the Wisconsin Tuberculosis (TB) Risk Assessment and Symptom Evaluation form.
Q: What is the purpose of Form F-02314?
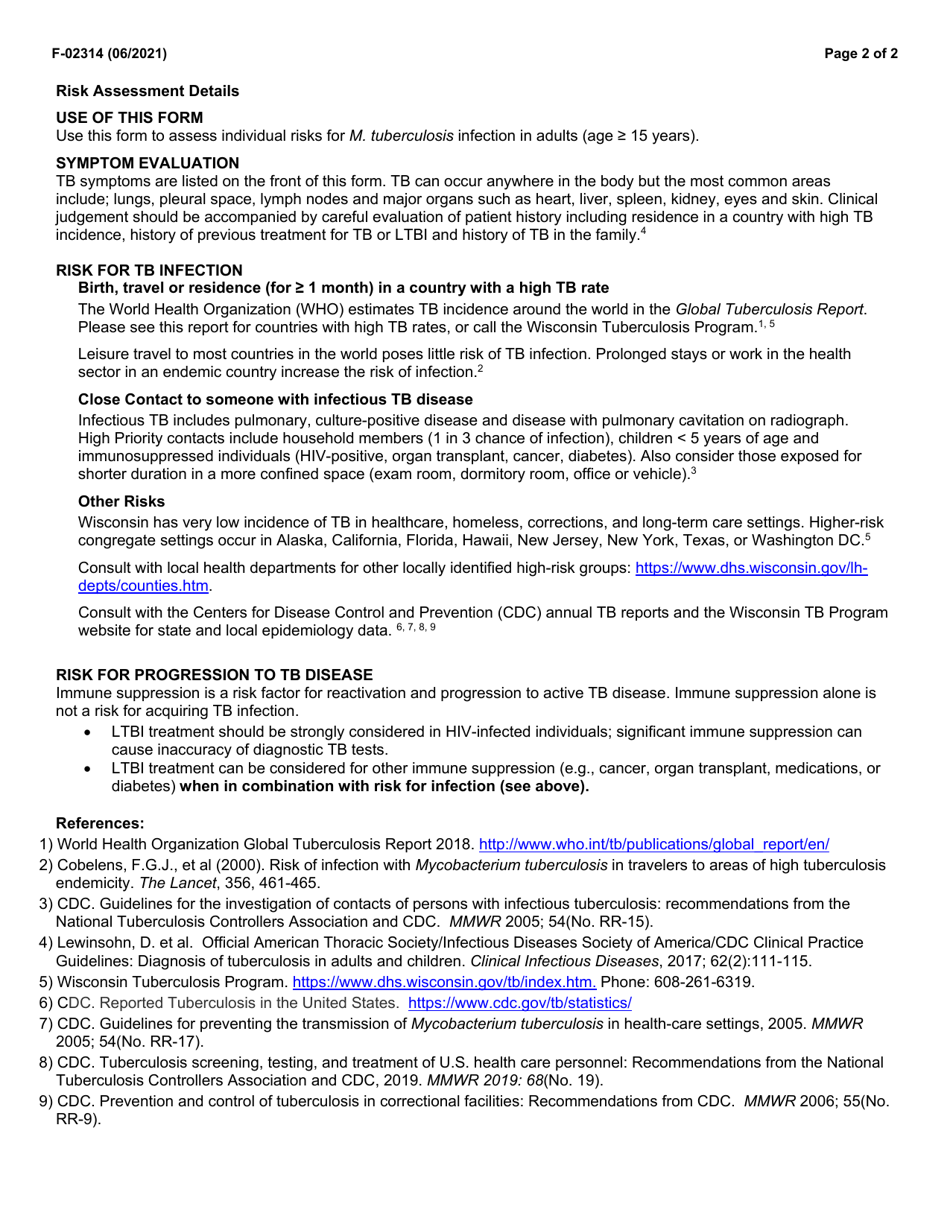
A: The purpose of Form F-02314 is to assess the risk of tuberculosis (TB) infection and evaluate symptoms related to TB.
Q: Who needs to fill out Form F-02314?
A: Form F-02314 needs to be filled out by individuals who are at risk of tuberculosis (TB) or who are experiencing symptoms related to TB.
Q: What information is required on Form F-02314?
A: Form F-02314 requires information about your personal and medical history, as well as any symptoms related to TB that you may be experiencing.
Q: Is Form F-02314 mandatory?
A: The completion of Form F-02314 may be required by healthcare providers or public health authorities in certain situations to assess TB risk.
Q: How often should I fill out Form F-02314?
A: The frequency of filling out Form F-02314 depends on your risk factors and the guidance of your healthcare provider or public health authorities.
Q: What should I do if I have symptoms related to TB?
A: If you have symptoms related to TB, you should contact a healthcare provider for further evaluation and testing.
Q: Is there a cost to fill out Form F-02314?
A: The cost of filling out Form F-02314 may vary depending on the healthcare provider or public health authority requirements.
Form Details:
- Released on June 1, 2021;
- The latest edition provided by the Wisconsin Department of Health Services;
- Easy to use and ready to print;
- Available in Spanish;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form F-02314 by clicking the link below or browse more documents and templates provided by the Wisconsin Department of Health Services.
Download Form F-02314 Wisconsin Tuberculosis (Tb) Risk Assessment and Symptom Evaluation - Wisconsin
1
2