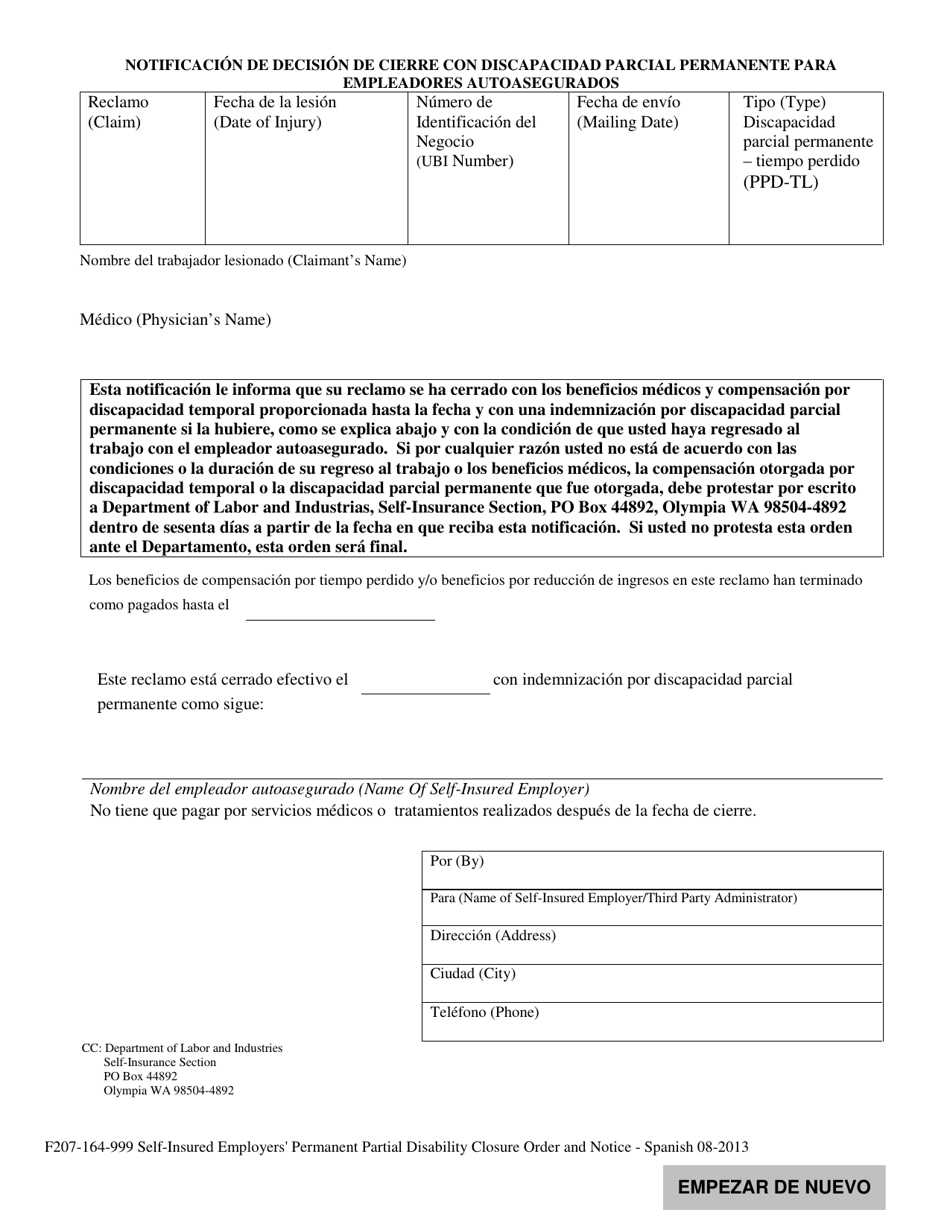
Formulario F207-164-999 Notificacion De Decision De Cierre Con Discapacidad Parcial Permanente Para Empleadores Autoasegurados - Washington (Spanish)
Qué es Formulario F207-164-999?
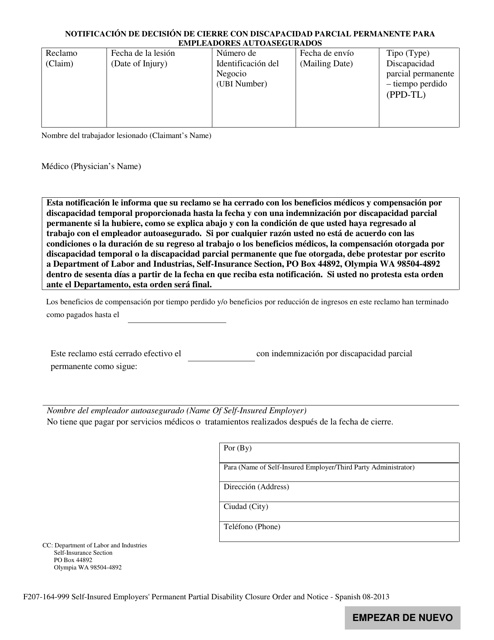
Este es un formulario legal que fue publicado por el Washington State Department of Labor and Industries, una autoridad gubernamental que opera dentro de Washington. A partir de hoy, el departamento emisor no proporciona en separado pautas de presentación para el formulario.
Detalles del formulario:
- Publicado el 1 de agosto de 2013;
- La última versión proporcionada por el Washington State Department of Labor and Industries;
- Lista para utilizar e imprimir;
- Fácil de personalizar;
- Compatible con la mayoría de las aplicaciones para visualizar PDF;
- Complete este formulario en línea.
Descargue una versión del Formulario F207-164-999 haciendo clic en el enlace debajo o busque más documentos y plantillas proporcionados por el Washington State Department of Labor and Industries.
FAQ
Q: What is Formulario F207-164-999?
A: Formulario F207-164-999 is a notification of decision letter for partial permanent disability closure for self-insured employers in Washington.
Q: What does the form notify about?
A: The form notifies the employer about the closure of a partial permanent disability claim.
Q: Who is the form intended for?
A: The form is intended for self-insured employers in Washington.
Q: What is a partial permanent disability?
A: A partial permanent disability is a permanent impairment that affects an individual's ability to work.
Q: What are self-insured employers?
A: Self-insured employers are those who manage workers' compensation claims on their own instead of purchasing insurance from a traditional insurer.