Form DCF-F-CFS2097 Kinship Care Payment Termination Notice - Wisconsin
What Is Form DCF-F-CFS2097?
This is a legal form that was released by the Wisconsin Department of Children and Families - a government authority operating within Wisconsin. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is Form DCF-F-CFS2097?
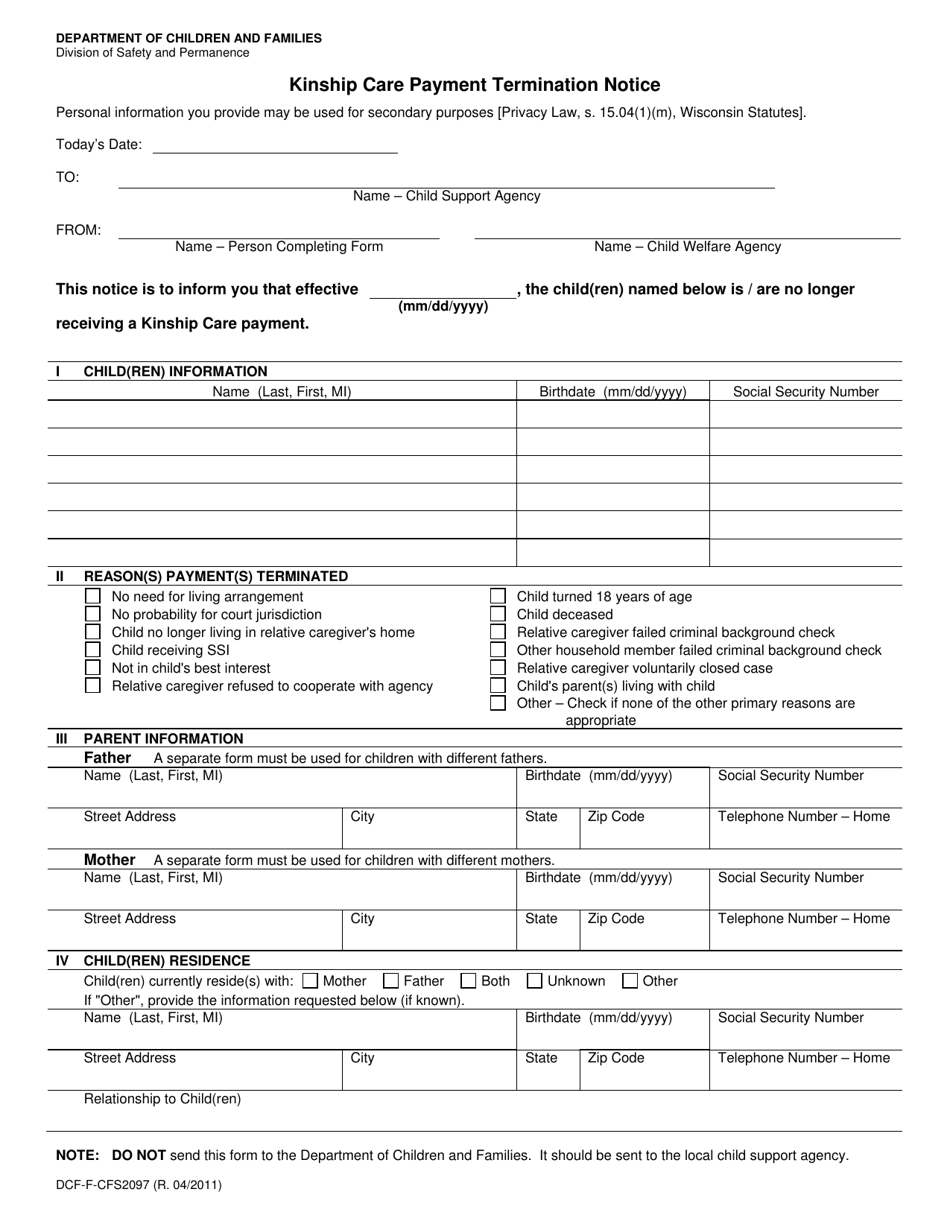
A: Form DCF-F-CFS2097 is a Kinship Care Payment Termination Notice in Wisconsin.
Q: What is Kinship Care?
A: Kinship Care refers to the care and custody of a child by a relative or non-relative extended family member.
Q: What is the purpose of Form DCF-F-CFS2097?
A: The purpose of Form DCF-F-CFS2097 is to notify the recipient that their kinship care payment is being terminated.
Q: Why would kinship care payments be terminated?
A: Kinship care payments may be terminated due to various reasons, such as changes in the child's living situation or eligibility criteria.
Q: Who receives the Form DCF-F-CFS2097?
A: The Form DCF-F-CFS2097 is typically received by the individual or family who is currently receiving kinship care payments.
Q: What should I do if I receive Form DCF-F-CFS2097?
A: If you receive Form DCF-F-CFS2097, you should review the notice carefully and follow any instructions provided, such as contacting the appropriate agency for further information or to request an appeal if necessary.
Q: Can I appeal the termination of kinship care payments?
A: Yes, you have the right to appeal the termination of kinship care payments. The notice should provide information on how to initiate an appeal.
Form Details:
- Released on April 1, 2011;
- The latest edition provided by the Wisconsin Department of Children and Families;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a printable version of Form DCF-F-CFS2097 by clicking the link below or browse more documents and templates provided by the Wisconsin Department of Children and Families.