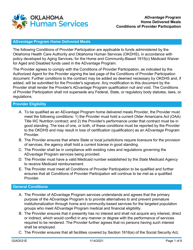
Form 02AD036E Amendment to the Conditions of Provider Participation for the Medicaid State Plan Personal Care Program - Oklahoma
What Is Form 02AD036E?
This is a legal form that was released by the Oklahoma Department of Human Services - a government authority operating within Oklahoma. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is Form 02AD036E?
A: Form 02AD036E is an amendment to the Conditions of Provider Participation for the Medicaid State Plan Personal Care Program in Oklahoma.
Q: What does this form do?
A: This form amends the Conditions of Provider Participation for the Medicaid State Plan Personal Care Program in Oklahoma.
Q: Who is this form for?
A: This form is for providers participating in the Medicaid State Plan Personal Care Program in Oklahoma.
Q: What is the Medicaid State Plan Personal Care Program?
A: The Medicaid State Plan Personal Care Program is a program that provides personal care services to eligible individuals in Oklahoma.
Q: What are the Conditions of Provider Participation?
A: The Conditions of Provider Participation are the requirements that providers must meet in order to participate in the Medicaid State Plan Personal Care Program in Oklahoma.
Q: Why would providers need to amend the Conditions of Provider Participation?
A: Providers may need to amend the Conditions of Provider Participation if there are changes to their eligibility or if they want to update their information.
Form Details:
- Released on January 14, 2021;
- The latest edition provided by the Oklahoma Department of Human Services;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form 02AD036E by clicking the link below or browse more documents and templates provided by the Oklahoma Department of Human Services.
Download Form 02AD036E Amendment to the Conditions of Provider Participation for the Medicaid State Plan Personal Care Program - Oklahoma
1
2

3