Release of Records Form
What Is a Release of Records Form?
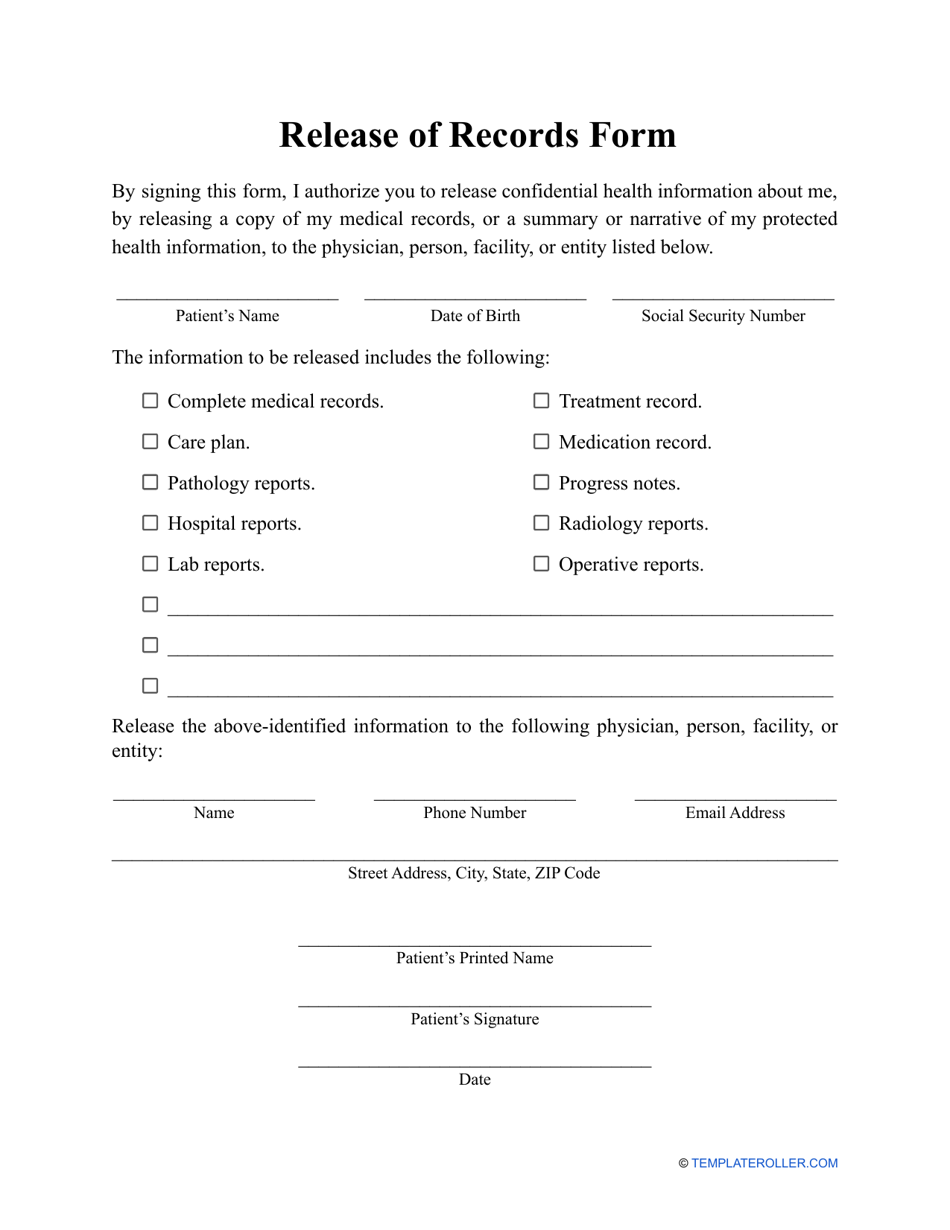
A Release of Records Form is a document that gives a patient permission to exchange their confidential medical records with other individuals or organizations. These can include family members, employers, insurance companies, or other health organizations.
Alternate Names:
- Records Release Form;
- Medical Records Release Form;
- Release of Medical Records Form.
A Medical Records Release Form template can be downloaded through the link below. The document allows the agreed parties to use the information provided for specific purposes. This protects patient confidentiality and also supports a medical professional as it will be confirmation that a patient has consented to their information being released.
A patient is within the right to make alterations or altogether terminate an existing Release of Records Form. If a parent wants to submit a form for a child, they have to prove that they are the legal guardian and submit a separate form for each child.
What Information Must Be Included on a Medical Records Release Form?
A generic Medical Records Release Form still needs to be specific. The following general information will need to be on every form regardless of the specifics:
- Information about the patient;
- Information about the current holder of the records;
- Information about who the records will be sent to;
- The authorized release time;
- The types of records that need to be released;
- Date of expiry (how long the document will be valid for). After this period, medical records will no longer be exchanged.
How to Fill Out a Medical Records Release Form?
Filling in the form is relatively simple, but making a small mistake can be costly as it will mean restarting the whole process again. Generally, you need to fill in the following parts:
- The personal details of the patient. Including their full name, date of birth, full address, information about any name changes during the requested period, telephone number, and their social security number.
- Specify the full name of the organization which currently possesses the records that you wish to disclose.
- The full name of the organization or person to which you intend to disclose your medical records.
- Details about the organization or person who will receive the records including their telephone number and address.
- Full list of the documents you want to be sent over. If you do not wish to disclose all your information, you have the right to share only some documents. You need to think about this carefully and list them. Usually, medical records hold information regarding your medical history, the medical history within your family, any treatments you have had, any results from genetic or laboratory testing, any prescribed medication that you are taking, details of any surgery or other medical procedures you have had along with their results and even information about your general lifestyle including whether or not you smoke or take drugs.
- You must also separately state if you are against information regarding HIV/AIDS or mental health-related records being released.
- Explain the purpose of the disclosure. Specify a time period for which the listed records will be shared. Only the documents you opted to share will be shared during this time period.
- Sign and date the document. If you are not the patient and signing for someone else, you must state their relationship to you and provide the relevant proof such as a death certificate (in case of death) or proof of guardianship if you are representing a child.
Not what you were looking for? Check out these related topics: