![]() This version of the form is not currently in use and is provided for reference only. Download this version of
Form HLTH5495
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
Form HLTH5495
for the current year.
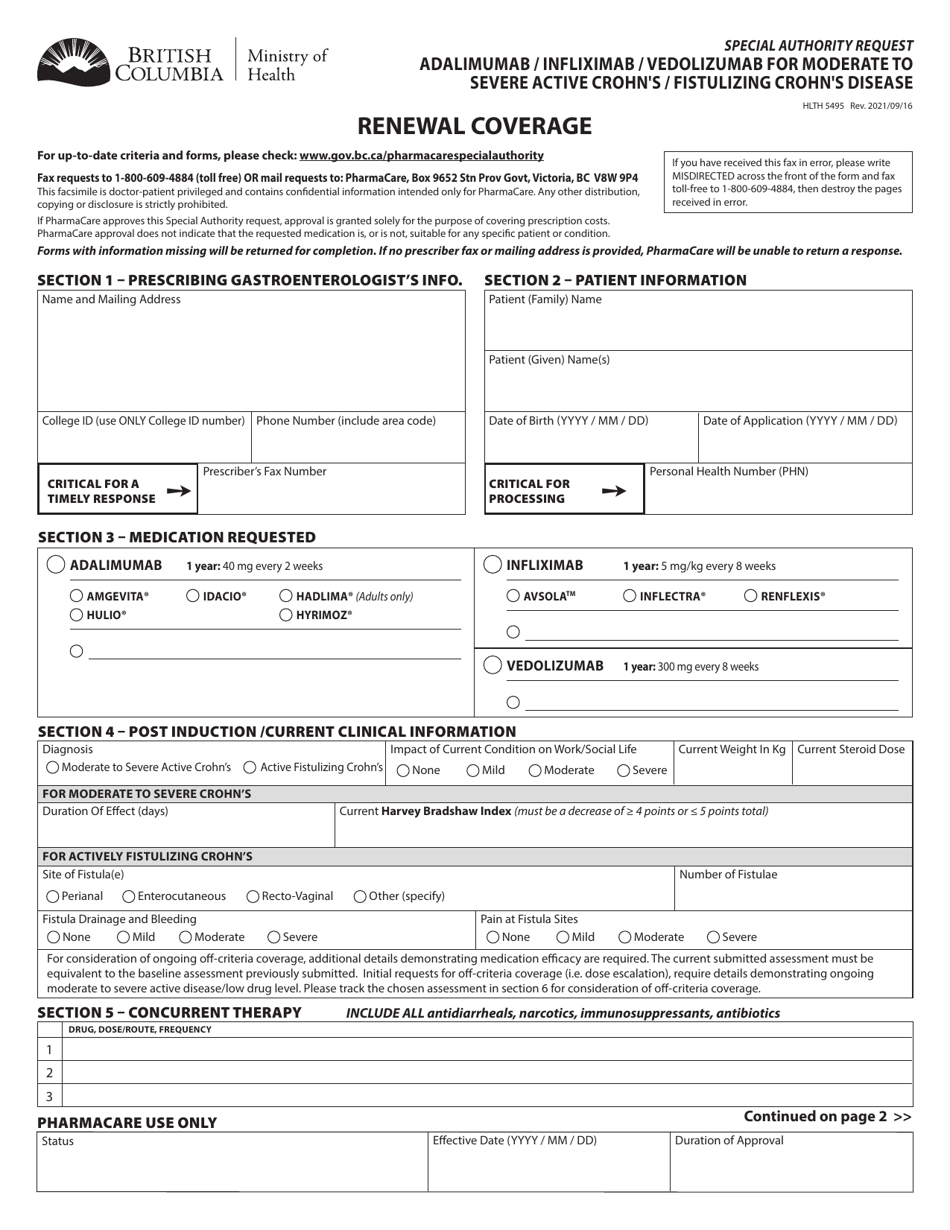
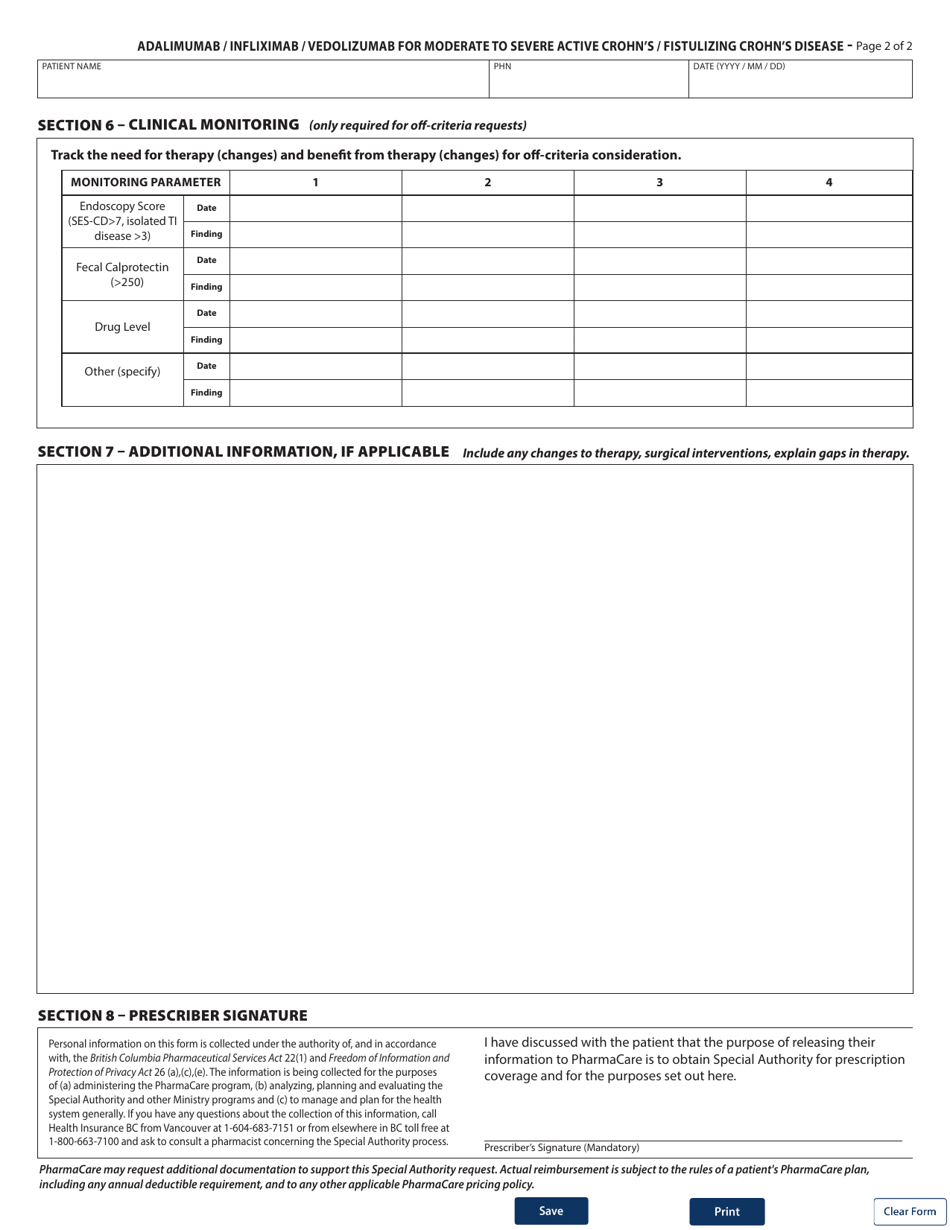
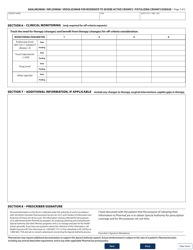
Form HLTH5495 Special Authority Request - Adalimumab / Infliximab / Vedolizumab for Moderate to Severe Active Crohn's / Fistulizing Crohn's Disease - Renewal Coverage - British Columbia, Canada
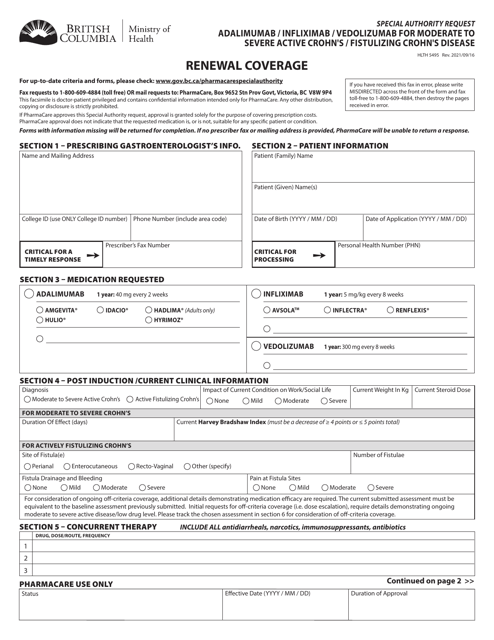
Form HLTH5495 is a special authority request form used in British Columbia, Canada for renewing coverage of medications (Adalimumab, Infliximab, and Vedolizumab) used to treat moderate to severe active Crohn's disease or fistulizing Crohn's disease. This form helps patients apply for continued coverage for these medications.
The patient or their authorized representative would generally file the Form HLTH5495 Special Authority Request - Adalimumab/Infliximab/Vedolizumab for Moderate to Severe Active Crohn's/Fistulizing Crohn's Disease - Renewal Coverage in British Columbia, Canada.
FAQ
Q: What is the purpose of Form HLTH5495?
A: Form HLTH5495 is used to request special authority for coverage of Adalimumab, Infliximab, or Vedolizumab for Moderate to Severe Active Crohn's/Fistulizing Crohn's Disease in British Columbia, Canada.
Q: Who can use Form HLTH5495?
A: This form can be used by healthcare providers in British Columbia, Canada to request renewal coverage for Adalimumab, Infliximab, or Vedolizumab for patients with Moderate to Severe Active Crohn's/Fistulizing Crohn's Disease.
Q: What conditions are eligible for coverage?
A: Form HLTH5495 is specifically for patients with Moderate to Severe Active Crohn's/Fistulizing Crohn's Disease.
Q: What medications are covered by this form?
A: This form covers Adalimumab, Infliximab, and Vedolizumab for the treatment of Moderate to Severe Active Crohn's/Fistulizing Crohn's Disease.
Q: Do I need to meet any criteria to be eligible for coverage?
A: Yes, patients must meet certain clinical criteria to be eligible for coverage. These criteria are outlined in the form.
Download Form HLTH5495 Special Authority Request - Adalimumab / Infliximab / Vedolizumab for Moderate to Severe Active Crohn's / Fistulizing Crohn's Disease - Renewal Coverage - British Columbia, Canada
1
2