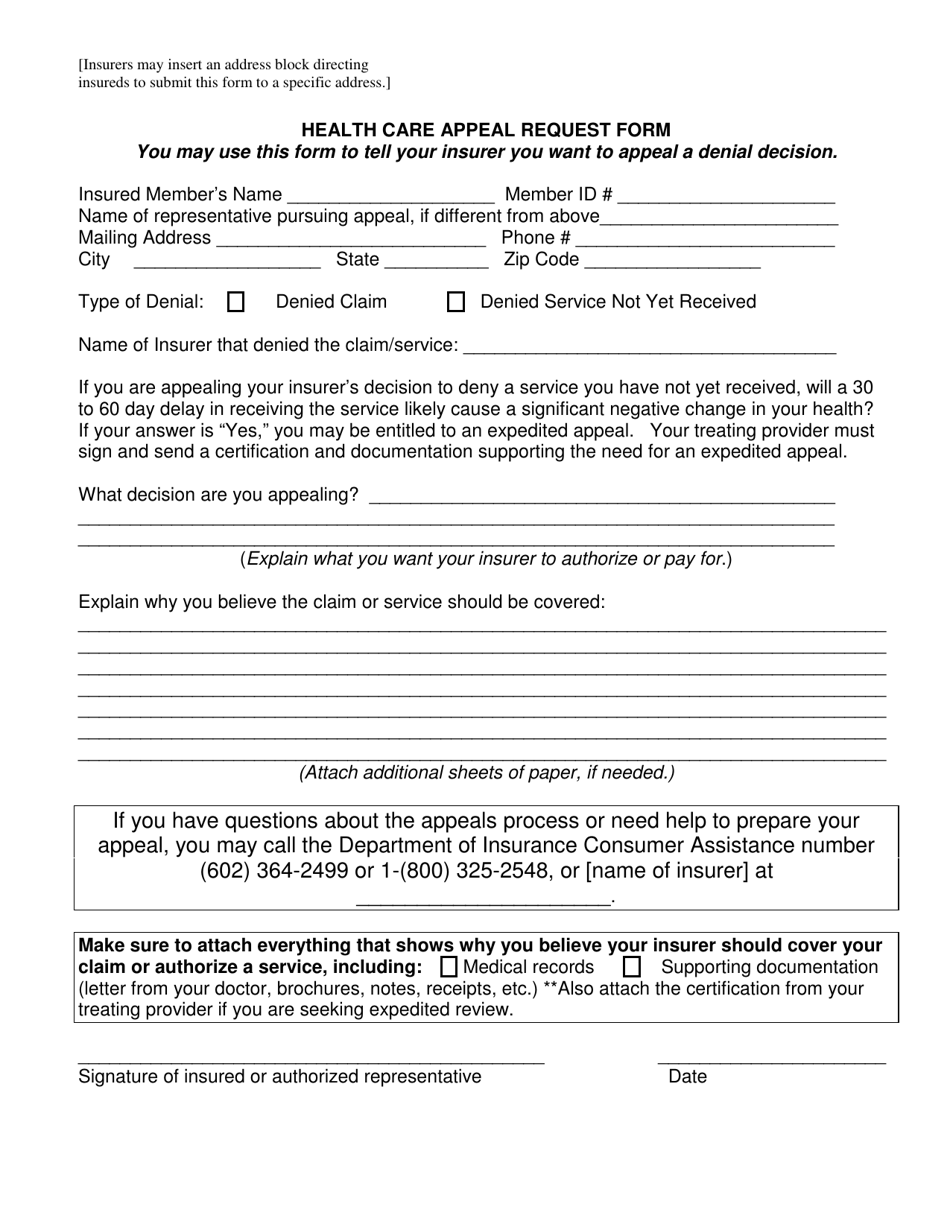
Health Care Appeal Request Form - Arizona
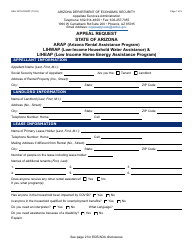
Health Care Appeal Request Form is a legal document that was released by the Arizona Department of Insurance and Financial Institutions - a government authority operating within Arizona.
FAQ
Q: What is a health care appeal request form?
A: A health care appeal request form is a document used to contest a decision made by your insurance company or health care provider.
Q: Why would I need to fill out a health care appeal request form?
A: You would need to fill out a health care appeal request form if you disagree with a decision made by your insurance company or health care provider and want to request a review or reconsideration of that decision.
Q: Is the health care appeal request form specific to Arizona?
A: Yes, the health care appeal request form mentioned is specific to Arizona.
Q: What information do I need to provide on the health care appeal request form?
A: You will need to provide your personal information, information about the decision you are appealing, and any supporting documentation related to your appeal.
Q: How long does it typically take to process a health care appeal request?
A: The processing time for a health care appeal request can vary, but it is generally within a specified timeframe set by your insurance company or health care provider.
Q: What happens after I submit a health care appeal request form?
A: After you submit a health care appeal request form, your request will be reviewed by the appropriate party, and you will be notified of the decision or outcome of the appeal.
Form Details:
- The latest edition currently provided by the Arizona Department of Insurance and Financial Institutions;
- Ready to use and print;
- Easy to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a printable version of the form by clicking the link below or browse more documents and templates provided by the Arizona Department of Insurance and Financial Institutions.