Form ODM03523 Request for Rx Prior Authorization - Ohio
What Is Form ODM03523?
This is a legal form that was released by the Ohio Department of Medicaid - a government authority operating within Ohio. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
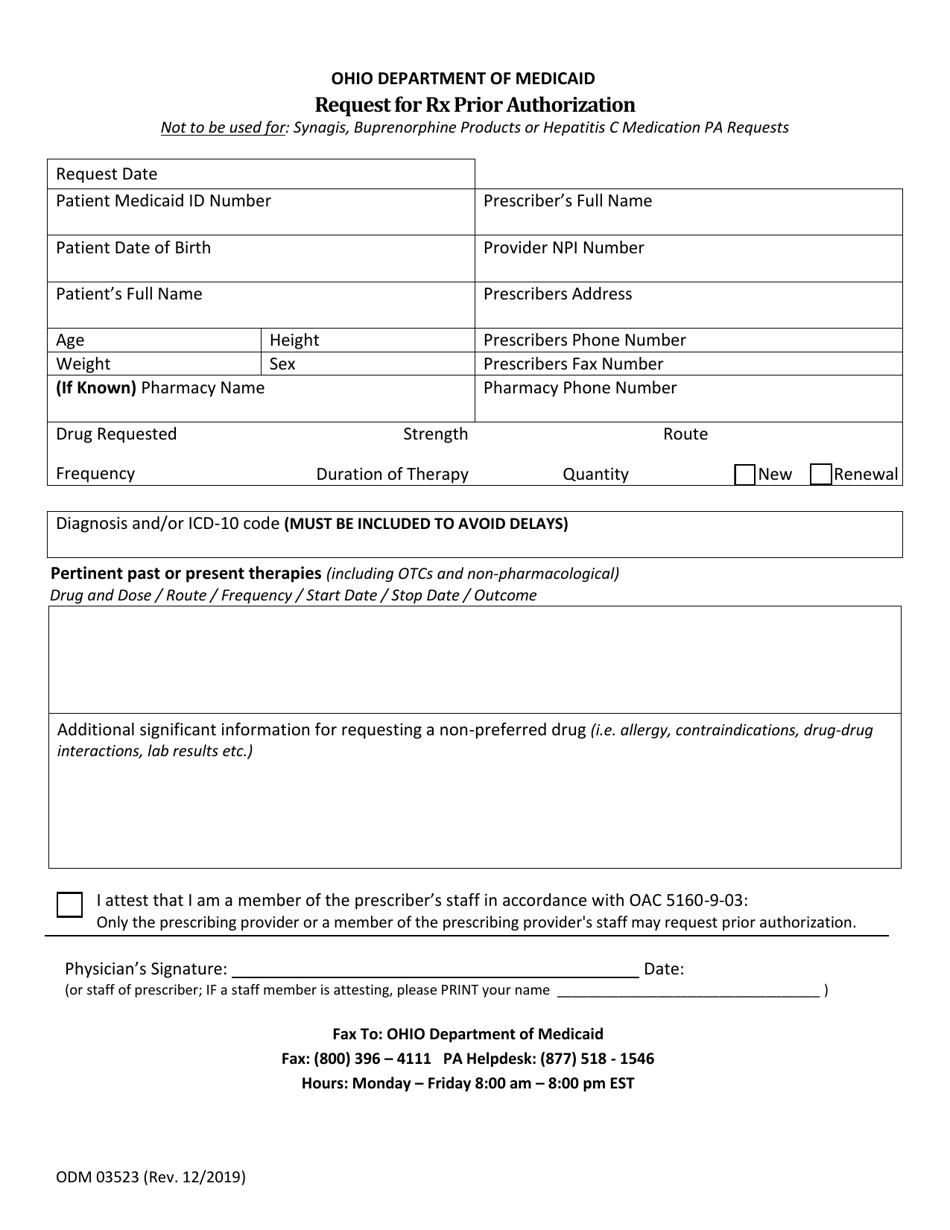
Q: What is ODM03523?
A: ODM03523 is a form used to request prior authorization for prescription medications in the state of Ohio.
Q: Why would I need to use ODM03523?
A: You would need to use ODM03523 if you want to obtain prior authorization for a prescription medication in Ohio.
Q: How do I fill out ODM03523?
A: You will need to provide your personal information, such as your name and address, as well as information about the prescribed medication and your healthcare provider.
Q: What should I do after filling out ODM03523?
A: After filling out ODM03523, you should submit the form to the Ohio Department of Medicaid or your healthcare provider for review and processing.
Q: Is there a fee for submitting ODM03523?
A: No, there is typically no fee for submitting ODM03523.
Q: How long does it take to get a decision on a prior authorization request using ODM03523?
A: The processing time for a prior authorization request can vary, but it typically takes a few business days to receive a decision.
Q: What happens if my prior authorization request is denied?
A: If your prior authorization request is denied, you may have options to appeal the decision or explore other medication options with your healthcare provider.
Q: Who can help me if I have questions about ODM03523?
A: If you have questions about ODM03523, you can reach out to the Ohio Department of Medicaid or your healthcare provider for assistance.
Form Details:
- Released on December 1, 2019;
- The latest edition provided by the Ohio Department of Medicaid;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form ODM03523 by clicking the link below or browse more documents and templates provided by the Ohio Department of Medicaid.