![]() This version of the form is not currently in use and is provided for reference only. Download this version of
Form ODM10239
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
Form ODM10239
for the current year.
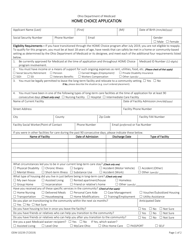
Form ODM10239 Home Choice Application - Ohio
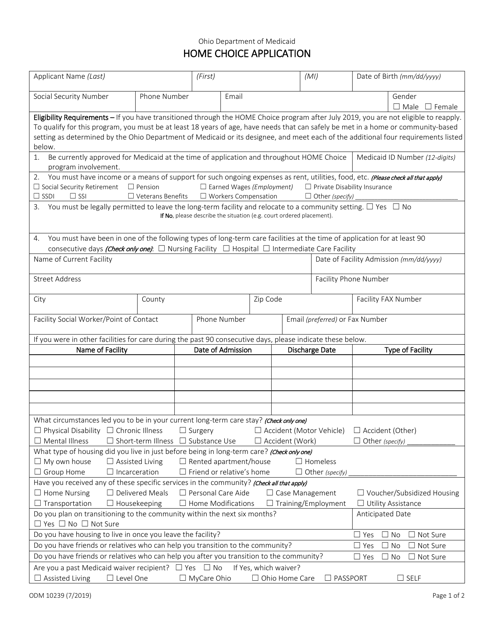
What Is Form ODM10239?
This is a legal form that was released by the Ohio Department of Medicaid - a government authority operating within Ohio. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is Form ODM10239?
A: Form ODM10239 is the Home Choice Application form for the state of Ohio.
Q: What is the purpose of Form ODM10239?
A: The purpose of Form ODM10239 is to apply for the Home Choice program in Ohio.
Q: What is the Home Choice program in Ohio?
A: The Home Choice program is a Medicaid program that helps individuals with disabilities and older adults transition from institutions to home and community-based settings.
Q: Who is eligible for the Home Choice program?
A: Eligibility for the Home Choice program is based on meeting certain criteria, including being a Medicaid recipient and requiring the level of care provided in an institution.
Q: Is there a fee to submit Form ODM10239?
A: No, there is no fee to submit Form ODM10239.
Q: What documents do I need to include with Form ODM10239?
A: You may need to include documents such as proof of income, proof of disability, and medical records with Form ODM10239. The specific requirements will be outlined in the instructions.
Q: How long does it take to process Form ODM10239?
A: The processing time for Form ODM10239 can vary, but it is typically completed within 45 days.
Q: Can I appeal if my application is denied?
A: Yes, if your application is denied, you have the right to appeal the decision. The appeal process will be outlined in the notification you receive.
Form Details:
- Released on July 1, 2019;
- The latest edition provided by the Ohio Department of Medicaid;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form ODM10239 by clicking the link below or browse more documents and templates provided by the Ohio Department of Medicaid.
Download Form ODM10239 Home Choice Application - Ohio
1
2