Form ODM10229 Certificate of Medical Necessity: High-Frequency Chest Wall Oscillation Devices - Ohio
What Is Form ODM10229?
This is a legal form that was released by the Ohio Department of Medicaid - a government authority operating within Ohio. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is Form ODM10229?
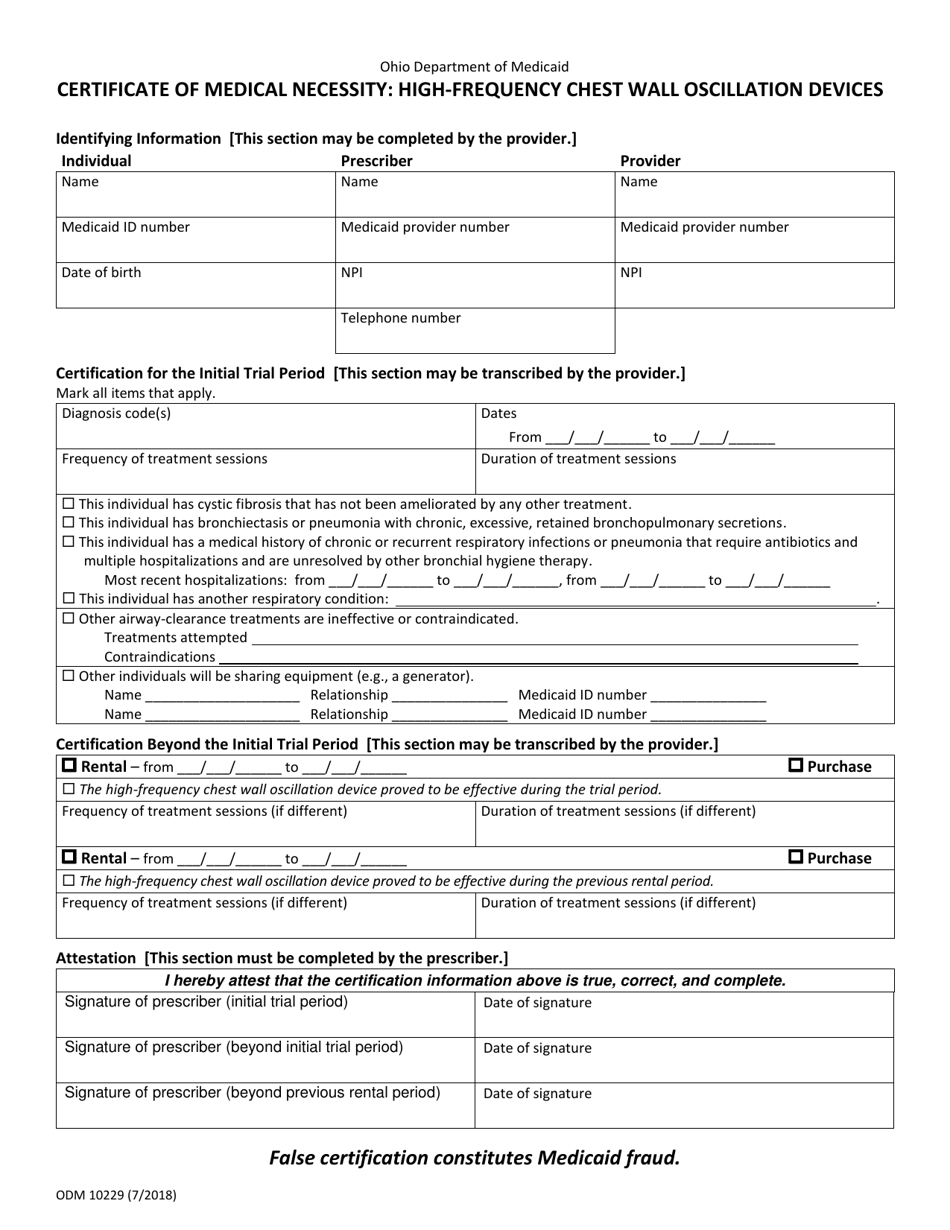
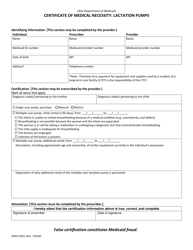
A: Form ODM10229 is the Certificate of Medical Necessity specifically for High-Frequency Chest Wall Oscillation Devices in the state of Ohio.
Q: What is a High-Frequency Chest Wall Oscillation Device?
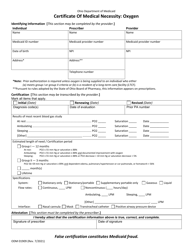
A: A High-Frequency Chest Wall Oscillation Device is a medical device used to help loosen and remove mucus from the lungs for individuals with breathing difficulties.
Q: Why is a Certificate of Medical Necessity needed for High-Frequency Chest Wall Oscillation Devices?
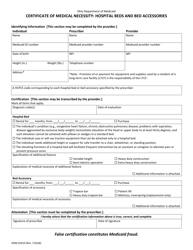
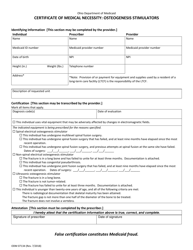
A: A Certificate of Medical Necessity is needed to provide documentation that the device is necessary for the individual's medical condition.
Q: Who needs to complete Form ODM10229?
A: The healthcare provider responsible for prescribing the High-Frequency Chest Wall Oscillation Device needs to complete and sign Form ODM10229.
Q: What information is required on Form ODM10229?
A: Form ODM10229 requires information about the patient, the healthcare provider, the medical condition, and the justification for the device's medical necessity.
Q: Is there a fee for submitting Form ODM10229?
A: No, there is no fee for submitting Form ODM10229.
Q: What should I do with the completed Form ODM10229?
A: After completing Form ODM10229, you should submit it to the Ohio Department of Medicaid for review and processing.
Form Details:
- Released on July 1, 2018;
- The latest edition provided by the Ohio Department of Medicaid;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form ODM10229 by clicking the link below or browse more documents and templates provided by the Ohio Department of Medicaid.