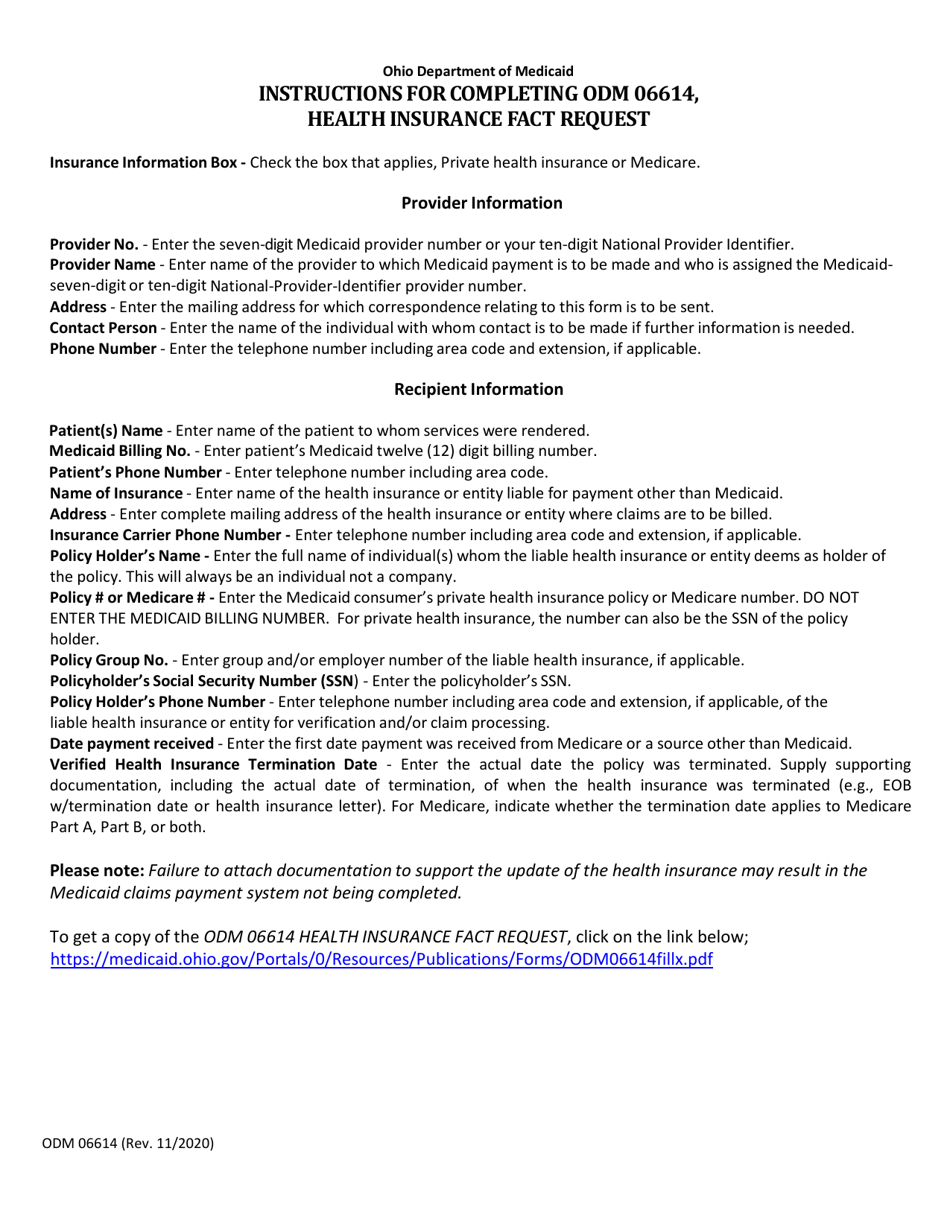
Instructions for Form ODM06614 Health Insurance Fact Request - Ohio
This document contains official instructions for Form ODM06614 , Health Insurance Fact Request - a form released and collected by the Ohio Department of Medicaid. An up-to-date fillable Form ODM06614 is available for download through this link.
FAQ
Q: What is Form ODM06614?
A: Form ODM06614 is a Health Insurance Fact Request form.
Q: Who is required to fill out Form ODM06614?
A: The form is to be filled out by residents of Ohio who need to request health insurance facts.
Q: What is the purpose of Form ODM06614?
A: The purpose of this form is to request information from health insurance companies about coverage, benefits, and other important details.
Q: Are there any fees associated with submitting Form ODM06614?
A: No, there are no fees for submitting this form.
Q: Is Form ODM06614 specific to Ohio?
A: Yes, Form ODM06614 is specific to the state of Ohio.
Q: What information do I need to provide on Form ODM06614?
A: You will need to provide your personal information, including your name, address, and contact details, as well as information about your current health insurance coverage.
Q: Can I request information on behalf of someone else?
A: Yes, you can request information on behalf of someone else, but you will need to provide their consent and include their information on the form.
Instruction Details:
- This 1-page document is available for download in PDF;
- Actual and applicable for the current year;
- Complete, printable, and free.
Download your copy of the instructions by clicking the link below or browse hundreds of other forms in our library of forms released by the Ohio Department of Medicaid.