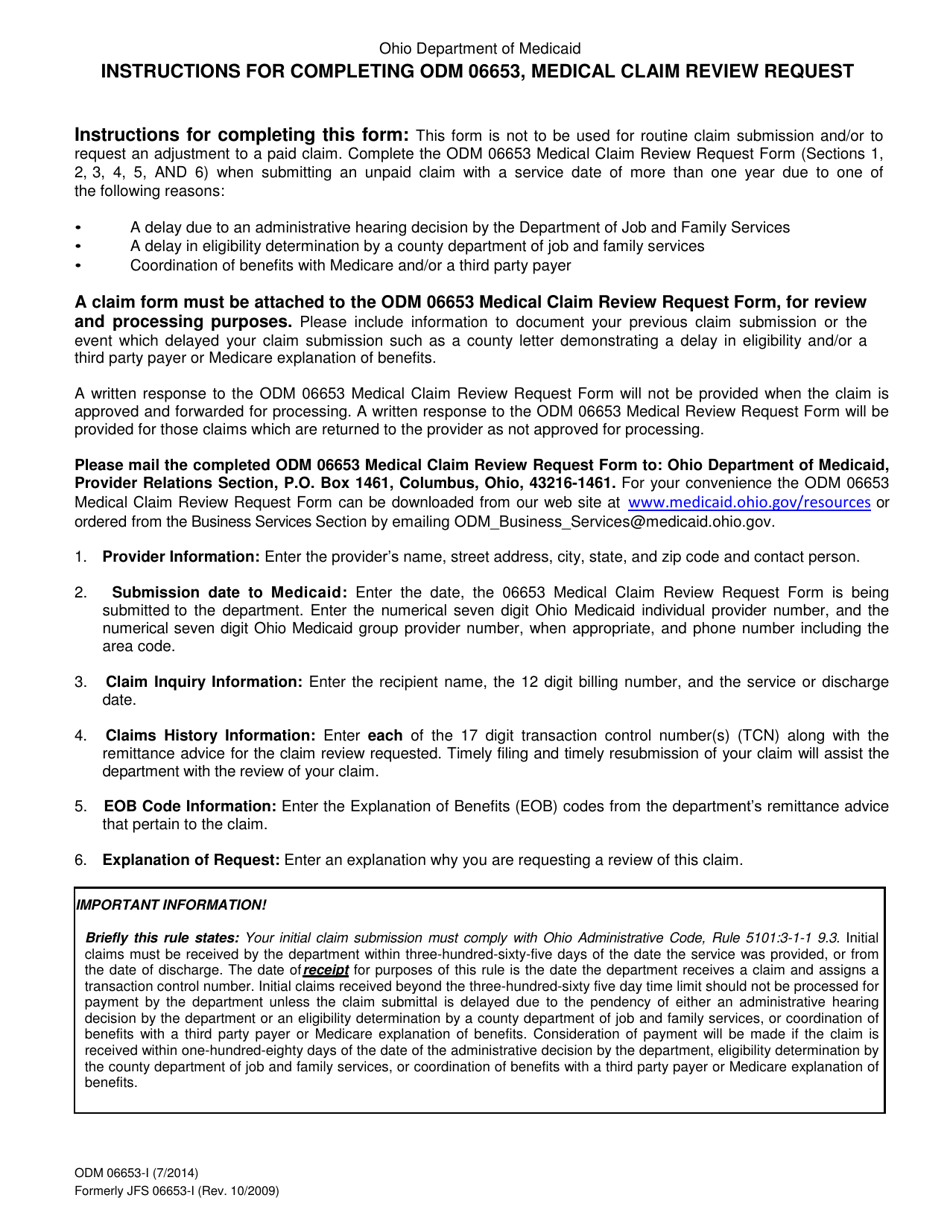
Instructions for Form ODM06653 Medical Claim Review Request - Ohio
This document contains official instructions for Form ODM06653 , Medical Claim Review Request - a form released and collected by the Ohio Department of Medicaid. An up-to-date fillable Form ODM06653 is available for download through this link.
FAQ
Q: What is Form ODM06653?
A: Form ODM06653 is a medical claim review request form used in Ohio.
Q: What is the purpose of Form ODM06653?
A: The purpose of Form ODM06653 is to request a review of a medical claim in Ohio.
Q: Who can use Form ODM06653?
A: Form ODM06653 can be used by individuals or their authorized representatives to request a review of a denied medical claim in Ohio.
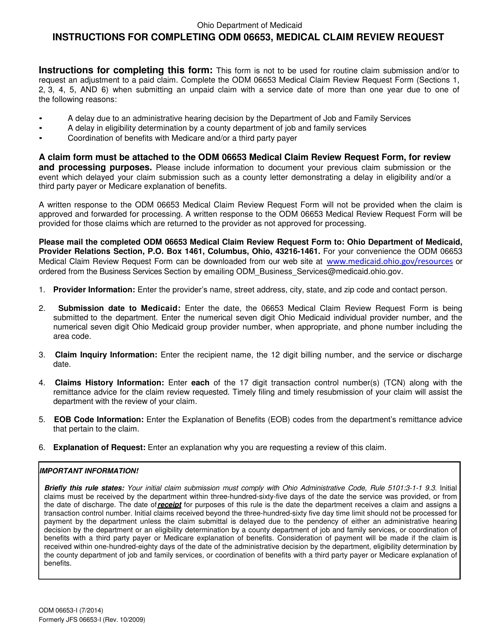
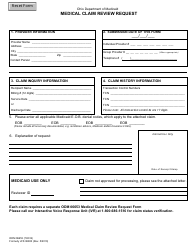
Q: What information is required on Form ODM06653?
A: Form ODM06653 requires information such as the patient's name, date of birth, Medicaid or insurance identification number, detailed description of services provided, and explanation of why the claim should be reviewed.
Q: Is there a deadline for submitting Form ODM06653?
A: Yes, there is a deadline for submitting Form ODM06653. The specific deadline may vary depending on the circumstances, so it is recommended to check the instructions on the form or contact the Ohio Department of Medicaid for more information.
Q: What should I do if my claim is denied after submitting Form ODM06653?
A: If your claim is denied after submitting Form ODM06653, you may have the option to appeal the decision. You should follow the appeal process outlined by the Ohio Department of Medicaid or your healthcare provider or insurance company.
Q: Can I get assistance in filling out Form ODM06653?
A: Yes, you can seek assistance from the Ohio Department of Medicaid or your healthcare provider or insurance company in filling out Form ODM06653.
Q: Are there any fees associated with submitting Form ODM06653?
A: There are no fees associated with submitting Form ODM06653.
Instruction Details:
- This 1-page document is available for download in PDF;
- Actual and applicable for the current year;
- Complete, printable, and free.
Download your copy of the instructions by clicking the link below or browse hundreds of other forms in our library of forms released by the Ohio Department of Medicaid.