![]() This version of the form is not currently in use and is provided for reference only. Download this version of
the document
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
the document
for the current year.
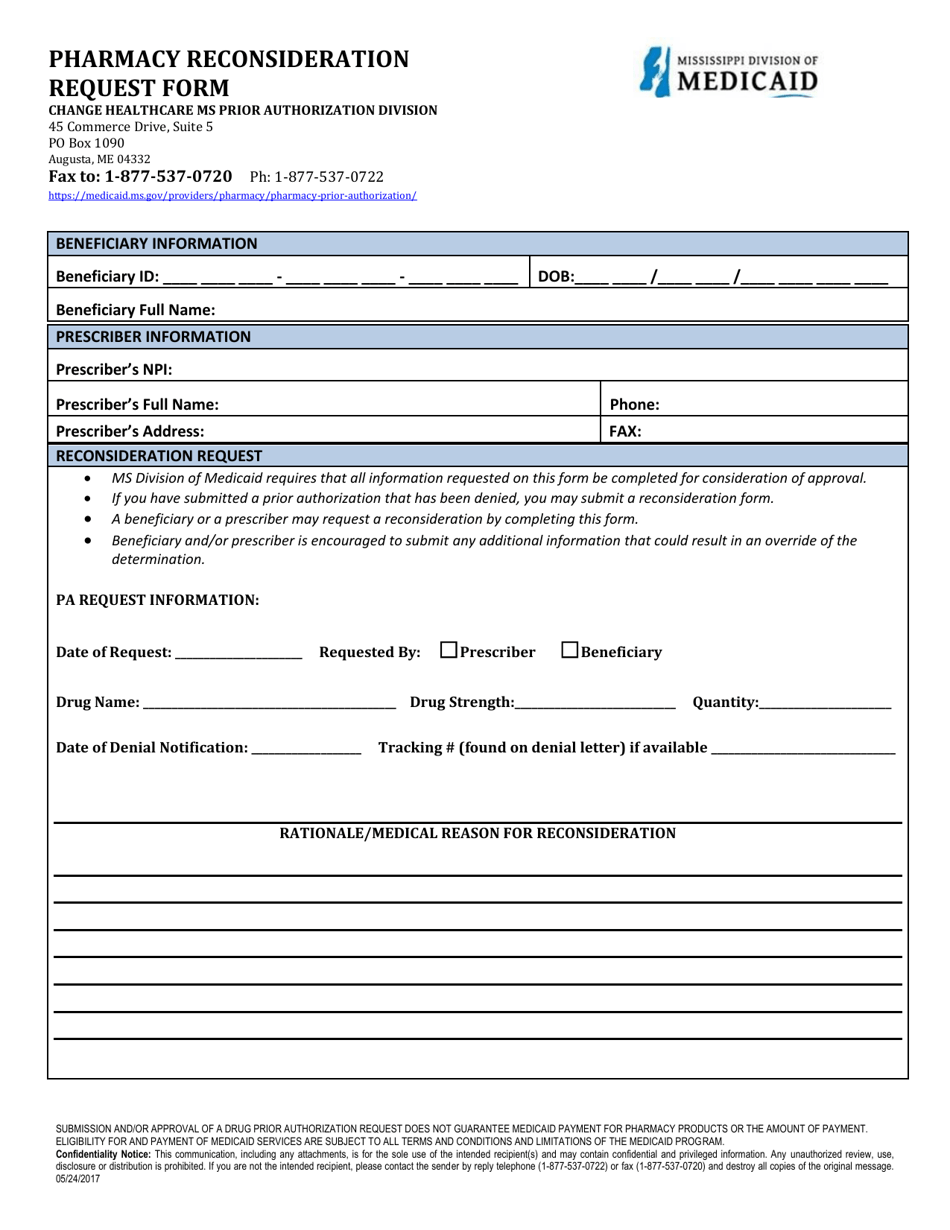
Pharmacy Reconsideration Request Form - Mississippi
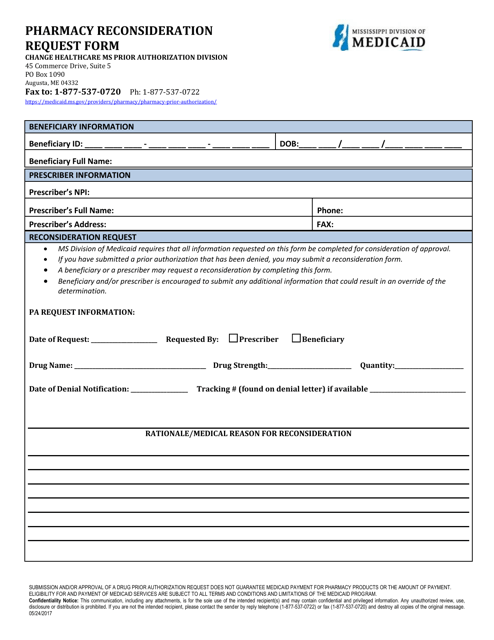
Pharmacy Reconsideration Request Form is a legal document that was released by the Mississippi Division of Medicaid - a government authority operating within Mississippi.
FAQ
Q: What is a Pharmacy Reconsideration Request Form?
A: A Pharmacy Reconsideration Request Form is a document used in Mississippi to request a review of a pharmacy claim or medication coverage decision.
Q: Who can use the Pharmacy Reconsideration Request Form?
A: The Pharmacy Reconsideration Request Form can be used by individuals who have been denied medication coverage or had a pharmacy claim rejected.
Q: How do I fill out the Pharmacy Reconsideration Request Form?
A: You will need to provide your personal information, including your name, address, and Medicaid identification number, as well as information about the medication and the reason for the request.
Q: What should I do after submitting the Pharmacy Reconsideration Request Form?
A: After submitting the form, you should receive a response from the Mississippi Department of Medicaid or your pharmacy benefits manager regarding the review of your request.
Form Details:
- Released on May 24, 2017;
- The latest edition currently provided by the Mississippi Division of Medicaid;
- Ready to use and print;
- Easy to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a printable version of the form by clicking the link below or browse more documents and templates provided by the Mississippi Division of Medicaid.