![]() This version of the form is not currently in use and is provided for reference only. Download this version of
Form C-251.1
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
Form C-251.1
for the current year.
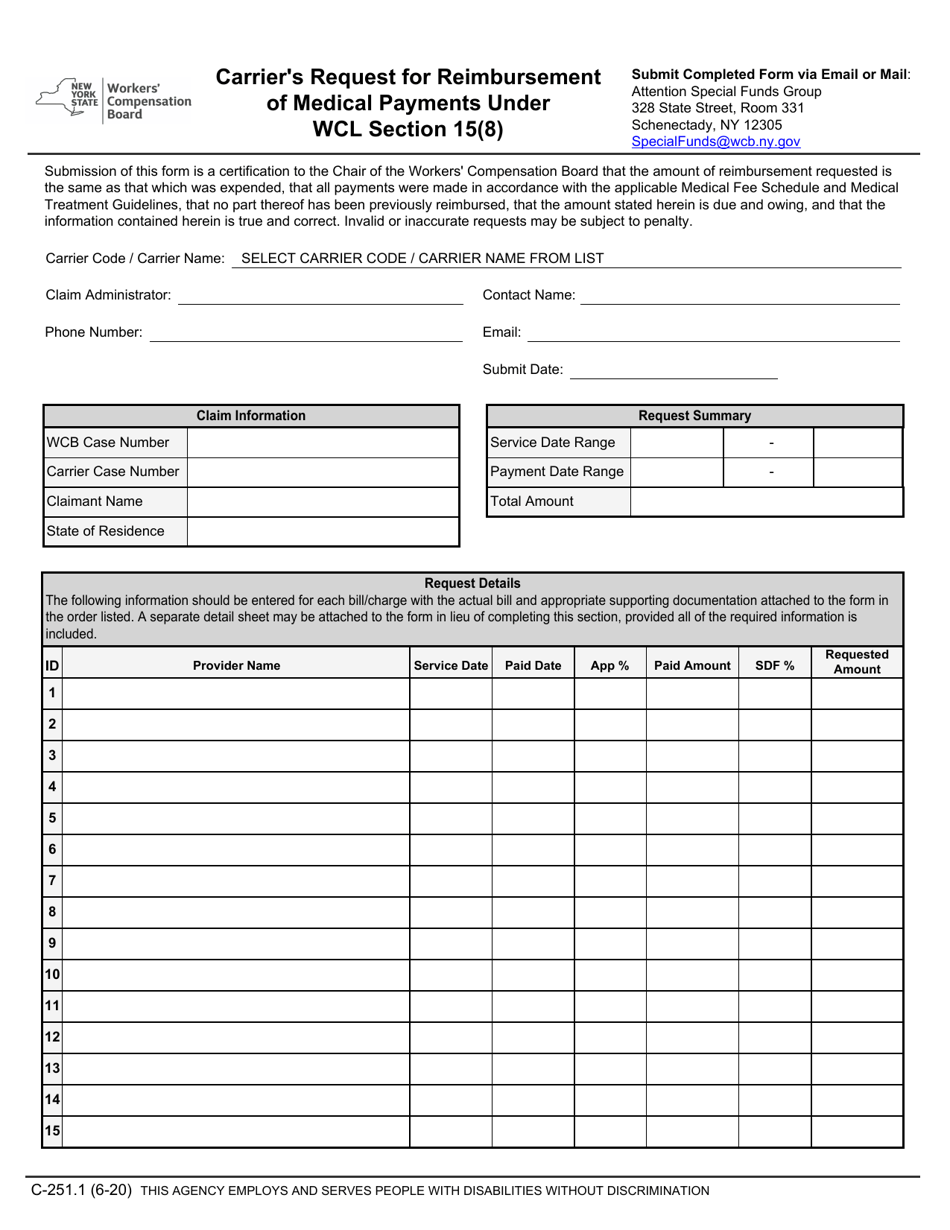
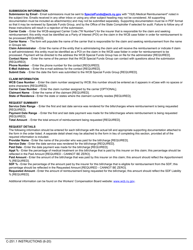
Form C-251.1 Carrier's Request for Reimbursement of Medical Payments Under Wcl Section 15(8) - New York
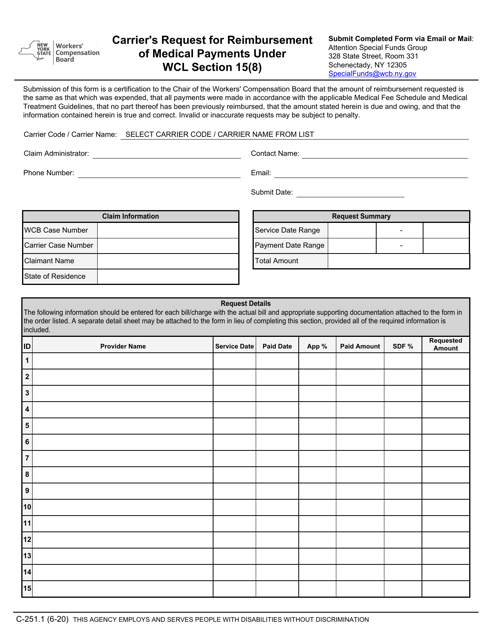
What Is Form C-251.1?
This is a legal form that was released by the New York State Workers' Compensation Board - a government authority operating within New York. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is Form C-251.1?
A: Form C-251.1 is called Carrier's Request for Reimbursement of Medical Payments under WCL Section 15(8).
Q: What is the purpose of Form C-251.1?
A: Form C-251.1 is used by carriers to request reimbursement of medical payments under WCL Section 15(8) in New York.
Q: Who can use Form C-251.1?
A: Carriers can use Form C-251.1 to request reimbursement of medical payments.
Q: What is WCL Section 15(8)?
A: WCL Section 15(8) refers to a section of the New York Workers' Compensation Law that relates to reimbursement of medical payments.
Form Details:
- Released on June 1, 2020;
- The latest edition provided by the New York State Workers' Compensation Board;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form C-251.1 by clicking the link below or browse more documents and templates provided by the New York State Workers' Compensation Board.
Download Form C-251.1 Carrier's Request for Reimbursement of Medical Payments Under Wcl Section 15(8) - New York
1
2