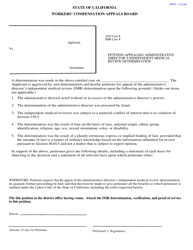
DWC Form IMR Application for Independent Medical Review - California
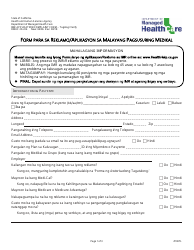
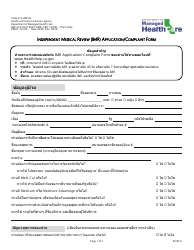
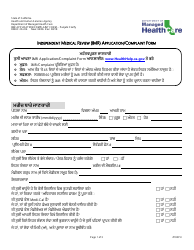
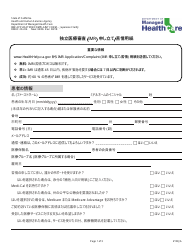
What Is DWC Form IMR?
This is a legal form that was released by the California Department of Industrial Relations - Division of Workers' Compensation - a government authority operating within California. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
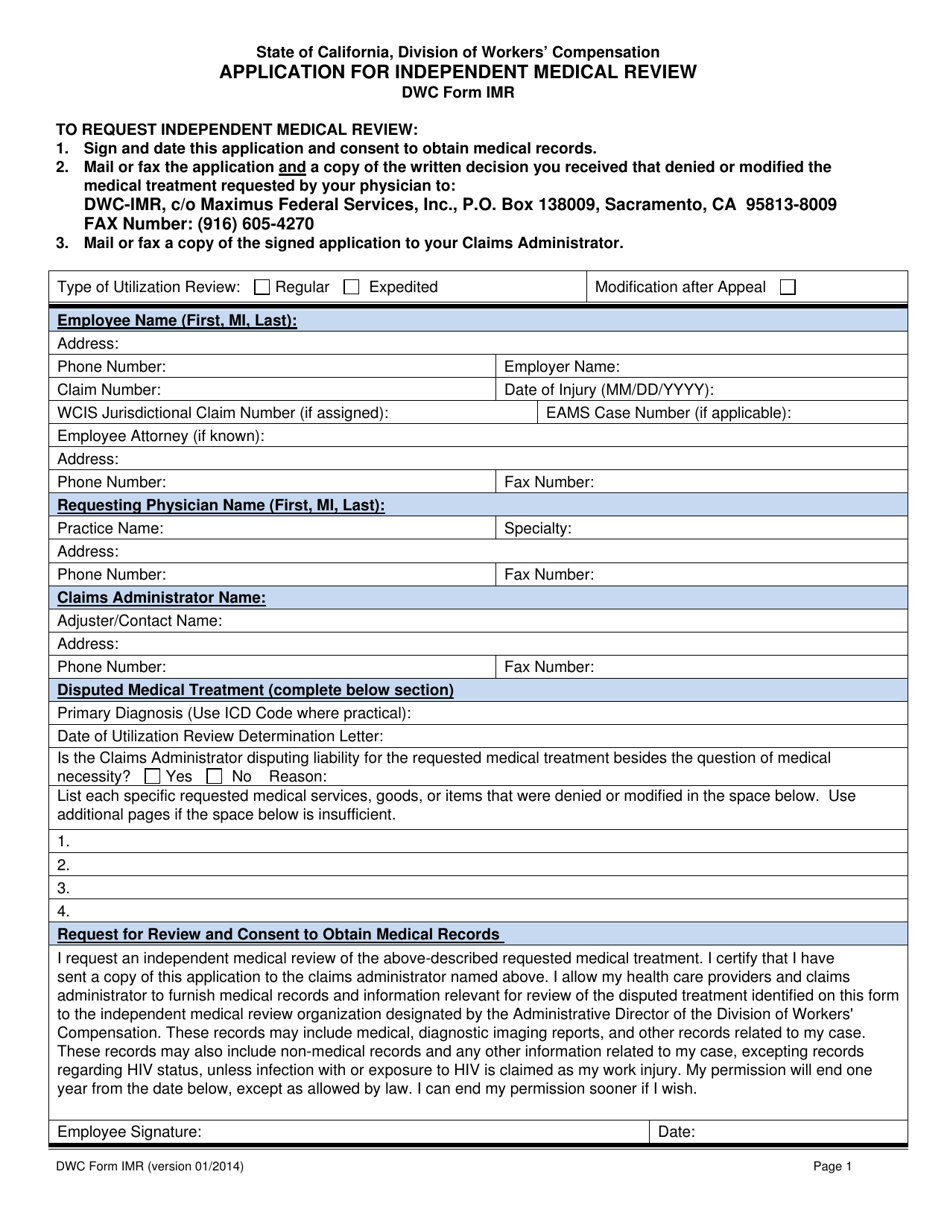
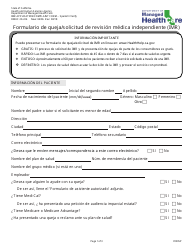
Q: What is DWC Form IMR?
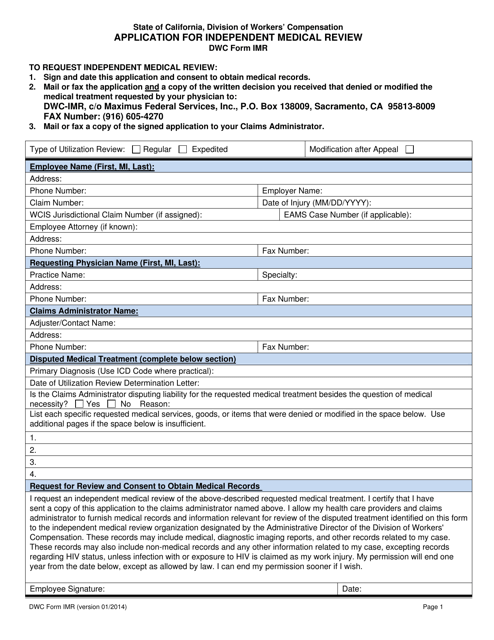
A: DWC Form IMR is an application for Independent Medical Review in California.
Q: What is the purpose of DWC Form IMR?
A: The purpose of DWC Form IMR is to request an independent medical review to resolve disputes regarding medical treatment or medical necessity.
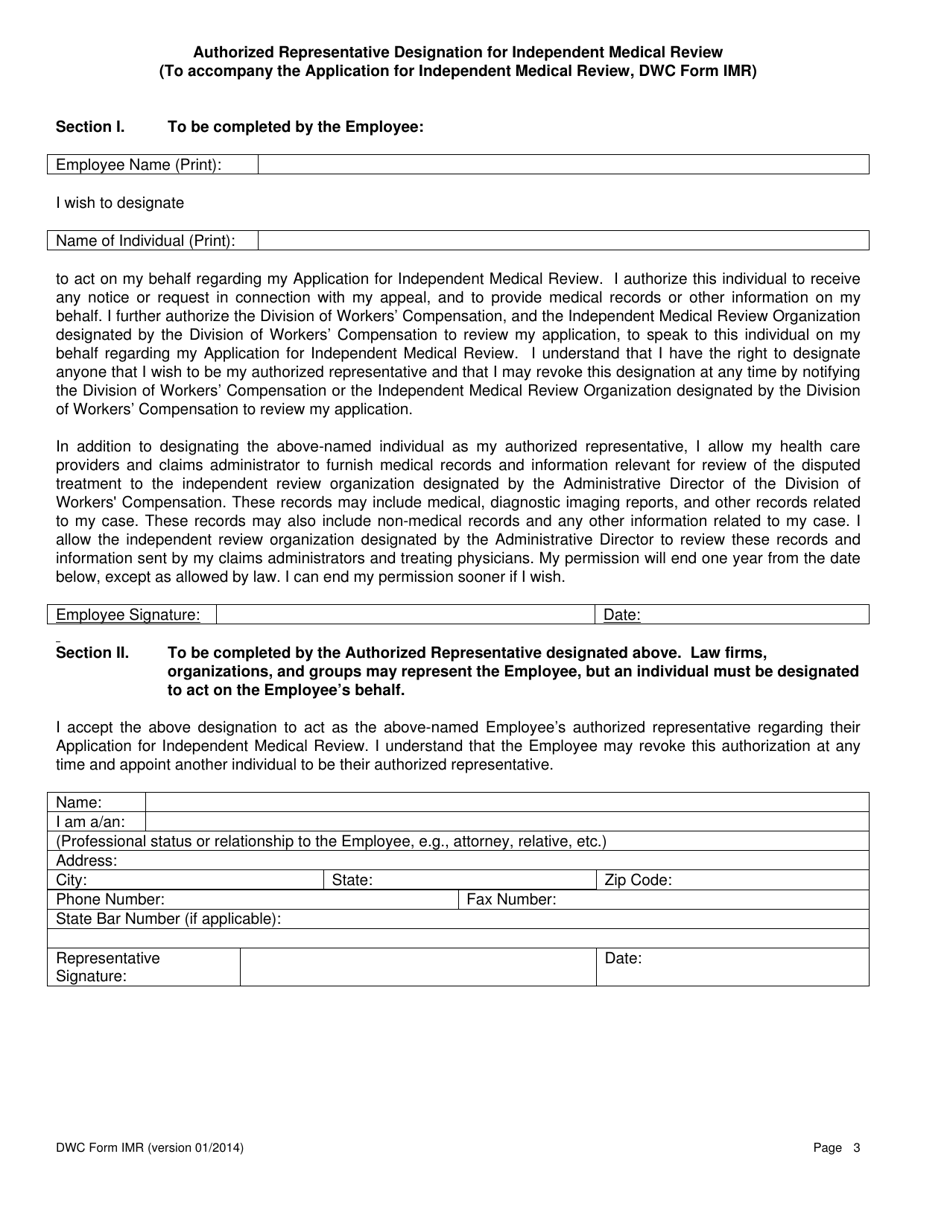
Q: Who can use DWC Form IMR?
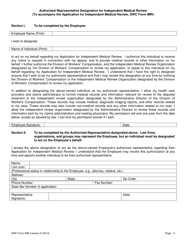
A: Any injured worker, employer, or claims administrator in California can use DWC Form IMR.
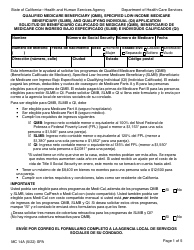
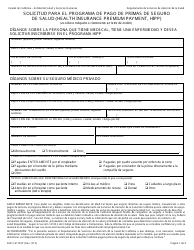
Q: What information is required on DWC Form IMR?
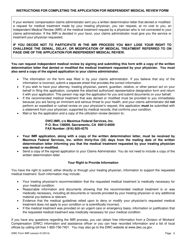
A: DWC Form IMR requires information such as your name, contact information, medical provider, and specific details about the disputed medical treatment.
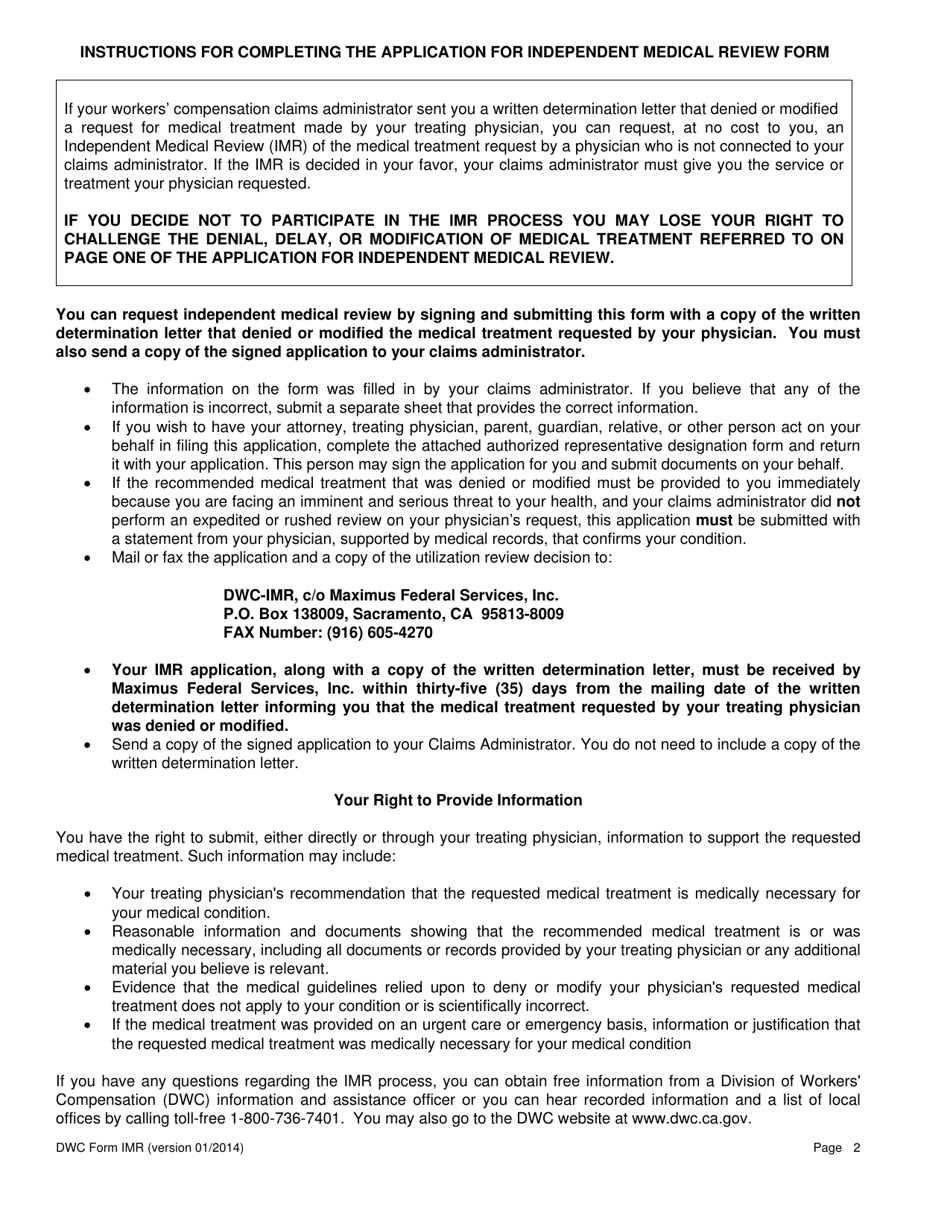
Q: What is the deadline for submitting DWC Form IMR?
A: The deadline for submitting DWC Form IMR is usually within 30 days of receiving the denial or modification of medical treatment.
Q: What happens after submitting DWC Form IMR?
A: After submitting DWC Form IMR, your case will be reviewed by an independent medical reviewer who will evaluate the medical evidence and make a determination.
Q: Can I appeal the decision made through DWC Form IMR?
A: No, the decision made through DWC Form IMR is final and binding.
Form Details:
- Released on January 1, 2014;
- The latest edition provided by the California Department of Industrial Relations - Division of Workers' Compensation;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a printable version of DWC Form IMR by clicking the link below or browse more documents and templates provided by the California Department of Industrial Relations - Division of Workers' Compensation.
Download DWC Form IMR Application for Independent Medical Review - California
1
2
3