![]() This version of the form is not currently in use and is provided for reference only. Download this version of
the document
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
the document
for the current year.
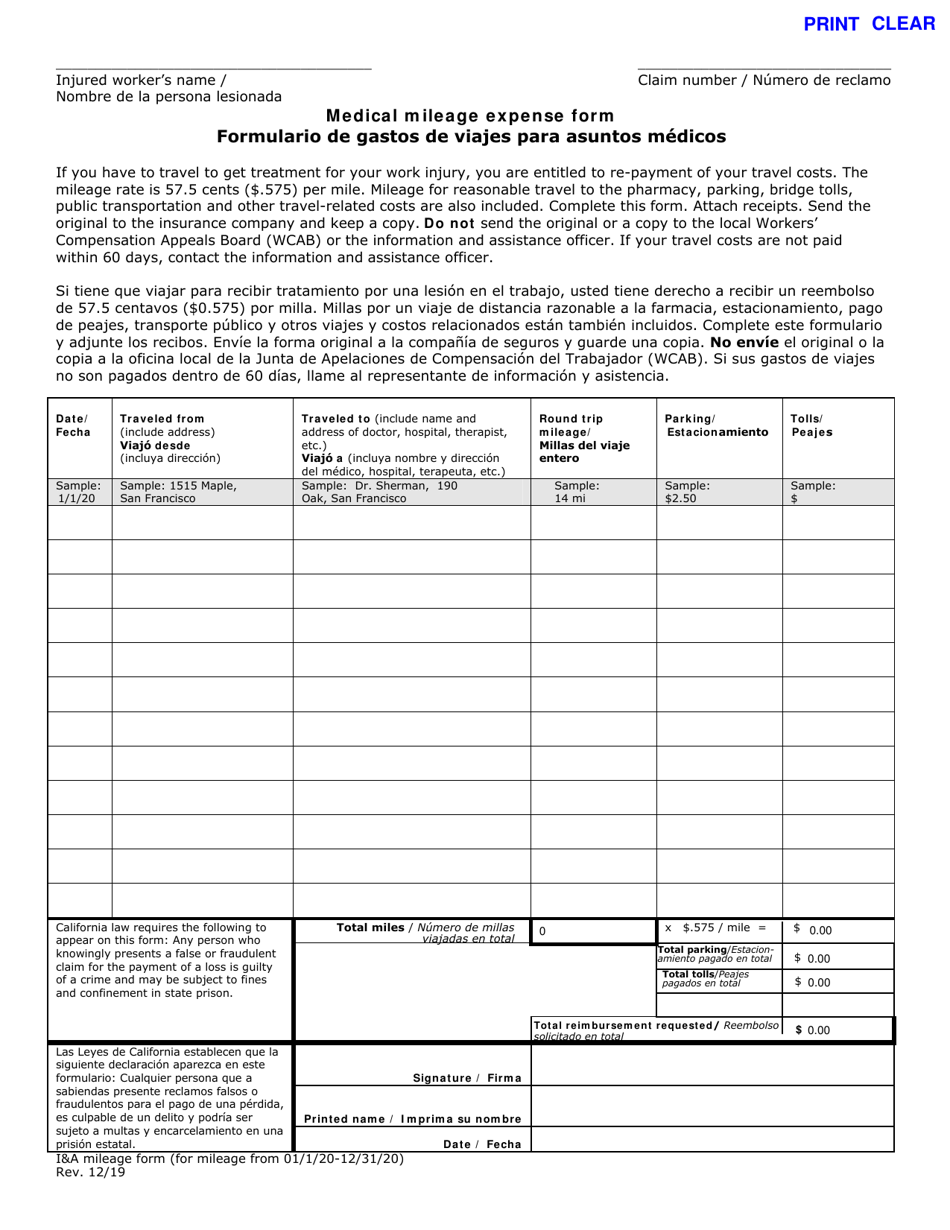
Medical Mileage Expense Form - California (English / Spanish)
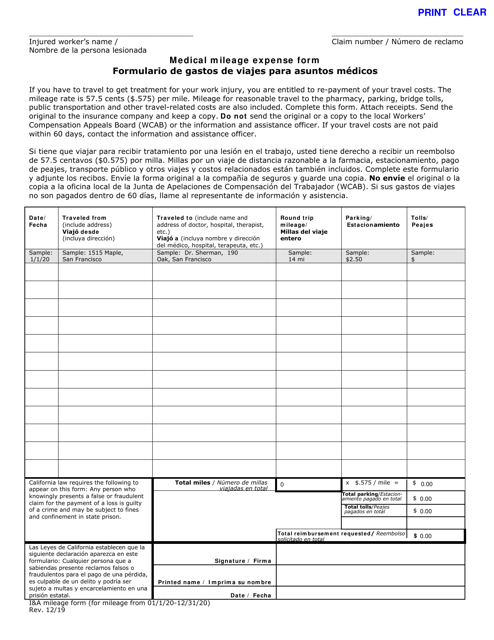
Medical Mileage Expense Form is a legal document that was released by the California Department of Industrial Relations - Division of Workers' Compensation - a government authority operating within California.
FAQ
Q: What is the Medical Mileage Expense Form?
A: The Medical Mileage Expense Form is a document used to claim reimbursement for travel expenses incurred for medical purposes.
Q: Who can use the Medical Mileage Expense Form?
A: Residents of California who have traveled for medical purposes can use this form to claim reimbursement for their travel expenses.
Q: What is the purpose of the form?
A: The purpose of the form is to provide a means for individuals to request reimbursement for mileage and related expenses when traveling for medical reasons.
Q: What expenses can be claimed using this form?
A: You can claim mileage expenses and related costs, such as parking fees and tolls, when traveling for medical purposes.
Q: Is there a deadline for submitting the form?
A: Yes, the form should be submitted within one year from the date the travel expenses were incurred.
Q: Who should I contact if I have questions about the form?
A: If you have any questions about the Medical Mileage Expense Form, you can contact the agency or organization responsible for approving the reimbursement.
Q: Is the form available in languages other than English and Spanish?
A: The provided document is available in both English and Spanish, but it may be available in additional languages depending on the specific jurisdiction.
Q: Can I use this form if I live outside of California?
A: No, this form is specifically for residents of California. If you live outside of California, you will need to check with your own state or jurisdiction for their specific reimbursement procedures.
Q: What documentation do I need to include with the form?
A: You will typically need to include supporting documentation such as receipts, medical records, or a letter from your healthcare provider to substantiate your claim for reimbursement.
Form Details:
- Released on December 1, 2019;
- The latest edition currently provided by the California Department of Industrial Relations - Division of Workers' Compensation;
- Ready to use and print;
- Easy to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of the form by clicking the link below or browse more documents and templates provided by the California Department of Industrial Relations - Division of Workers' Compensation.