Form 3039 Authorization to Disclose Protected Health Information - Texas
What Is Form 3039?
This is a legal form that was released by the Texas Health and Human Services - a government authority operating within Texas. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is Form 3039?
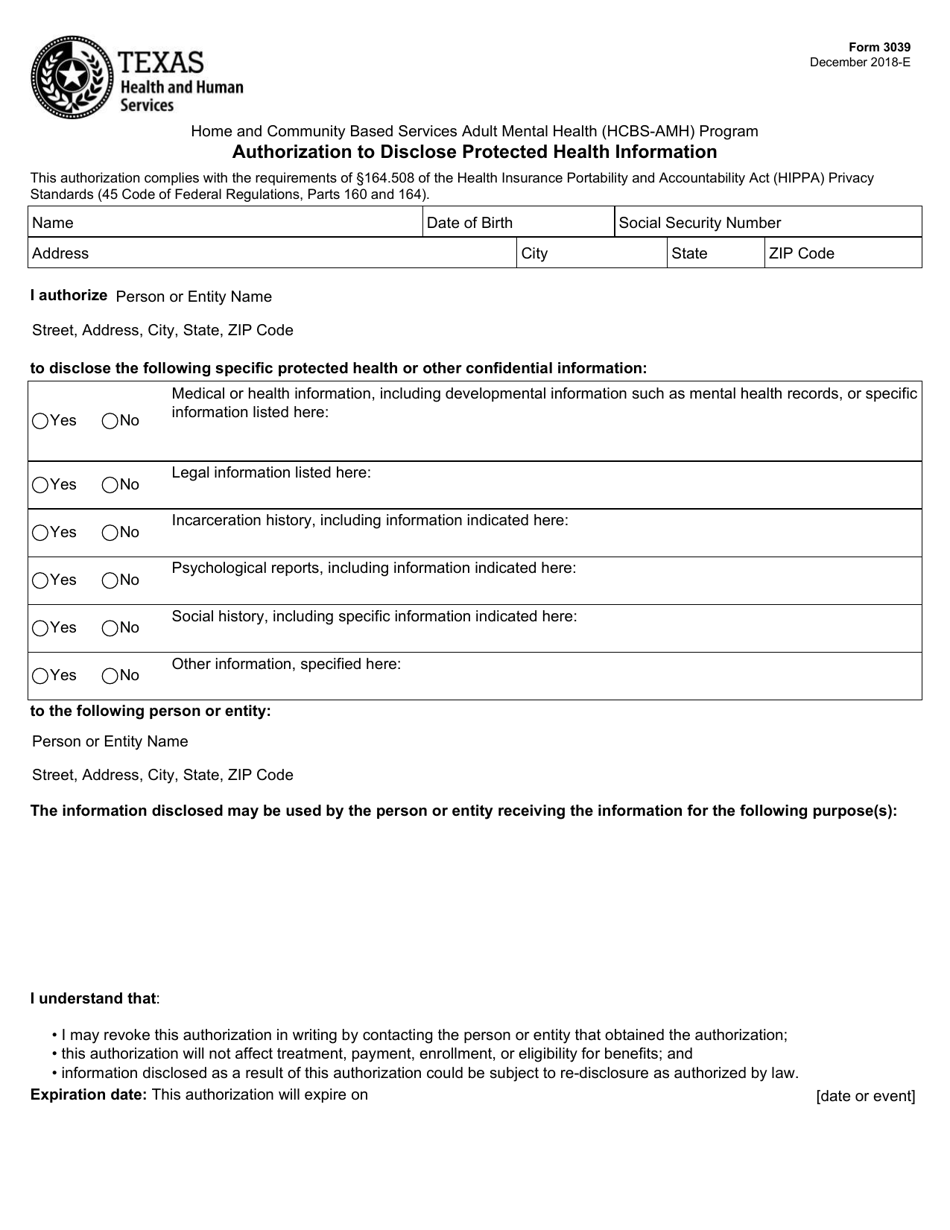
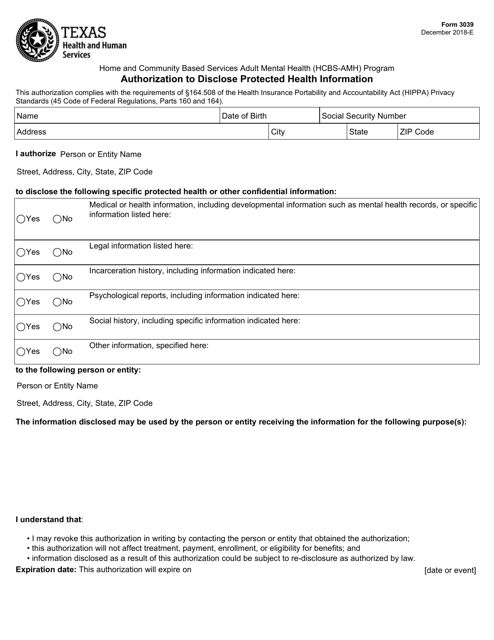
A: Form 3039 is the Authorization to Disclose Protected Health Information (PHI) in Texas.
Q: What is the purpose of Form 3039?
A: The purpose of Form 3039 is to obtain patient consent to disclose their protected health information to others.
Q: Who needs to fill out Form 3039?
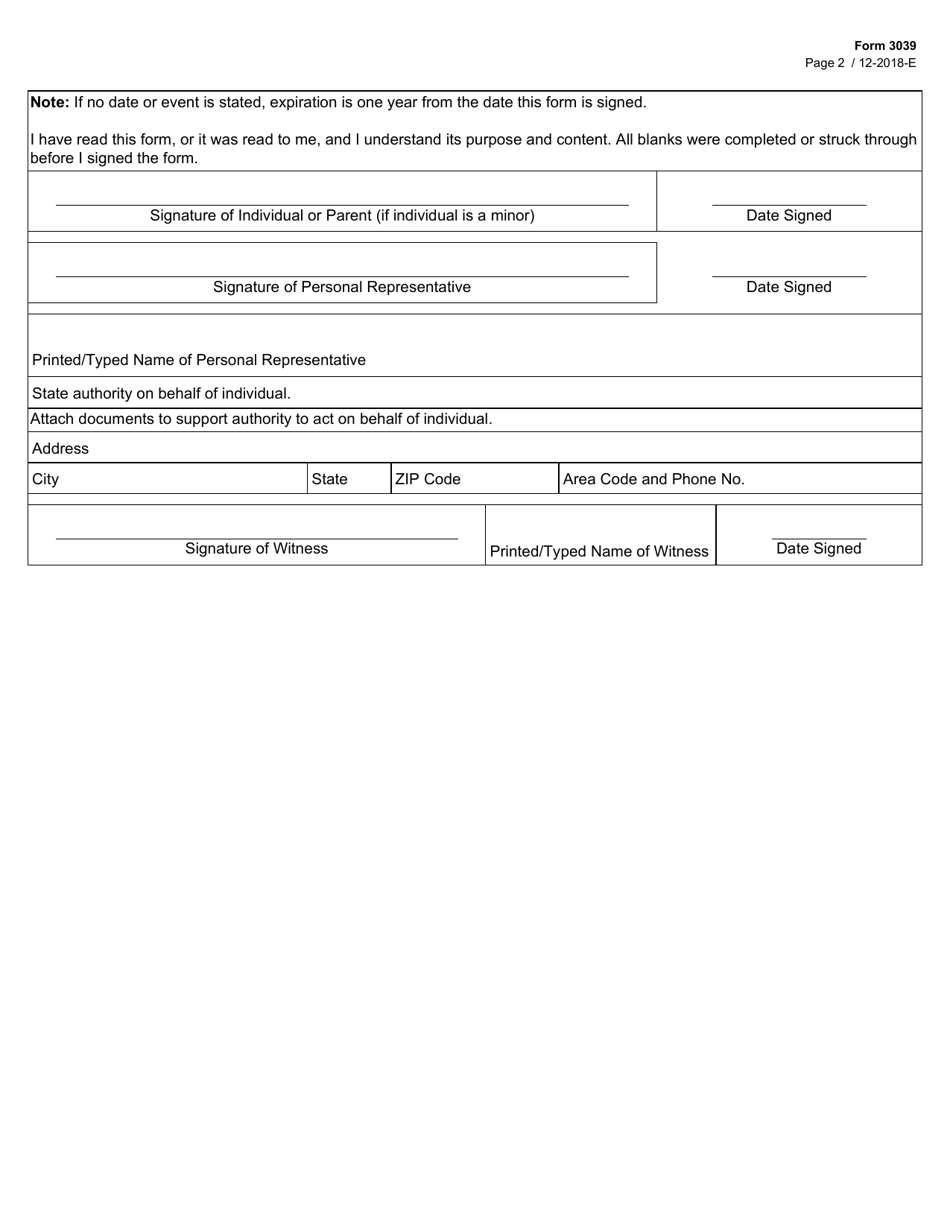
A: The patient or their legal representative needs to fill out Form 3039.
Q: What information is required on Form 3039?
A: Form 3039 requires the patient's name, date of birth, contact information, the information to be disclosed, and the purpose of the disclosure.
Q: Are there any fees associated with submitting Form 3039?
A: No, there are no fees associated with submitting Form 3039.
Q: What happens after Form 3039 is submitted?
A: After Form 3039 is submitted, the healthcare provider can disclose the patient's protected health information as authorized.
Q: How long is Form 3039 valid for?
A: Form 3039 is valid for one year from the date it is signed, unless a different time period is specified.
Q: Can Form 3039 be revoked?
A: Yes, the patient or their legal representative can revoke Form 3039 at any time.
Q: Is Form 3039 specific to Texas?
A: Yes, Form 3039 is specific to Texas and follows the state's laws and regulations regarding the disclosure of protected health information.
Form Details:
- Released on December 1, 2018;
- The latest edition provided by the Texas Health and Human Services;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form 3039 by clicking the link below or browse more documents and templates provided by the Texas Health and Human Services.
Download Form 3039 Authorization to Disclose Protected Health Information - Texas
1
2