![]() This version of the form is not currently in use and is provided for reference only. Download this version of
Form 1347
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
Form 1347
for the current year.
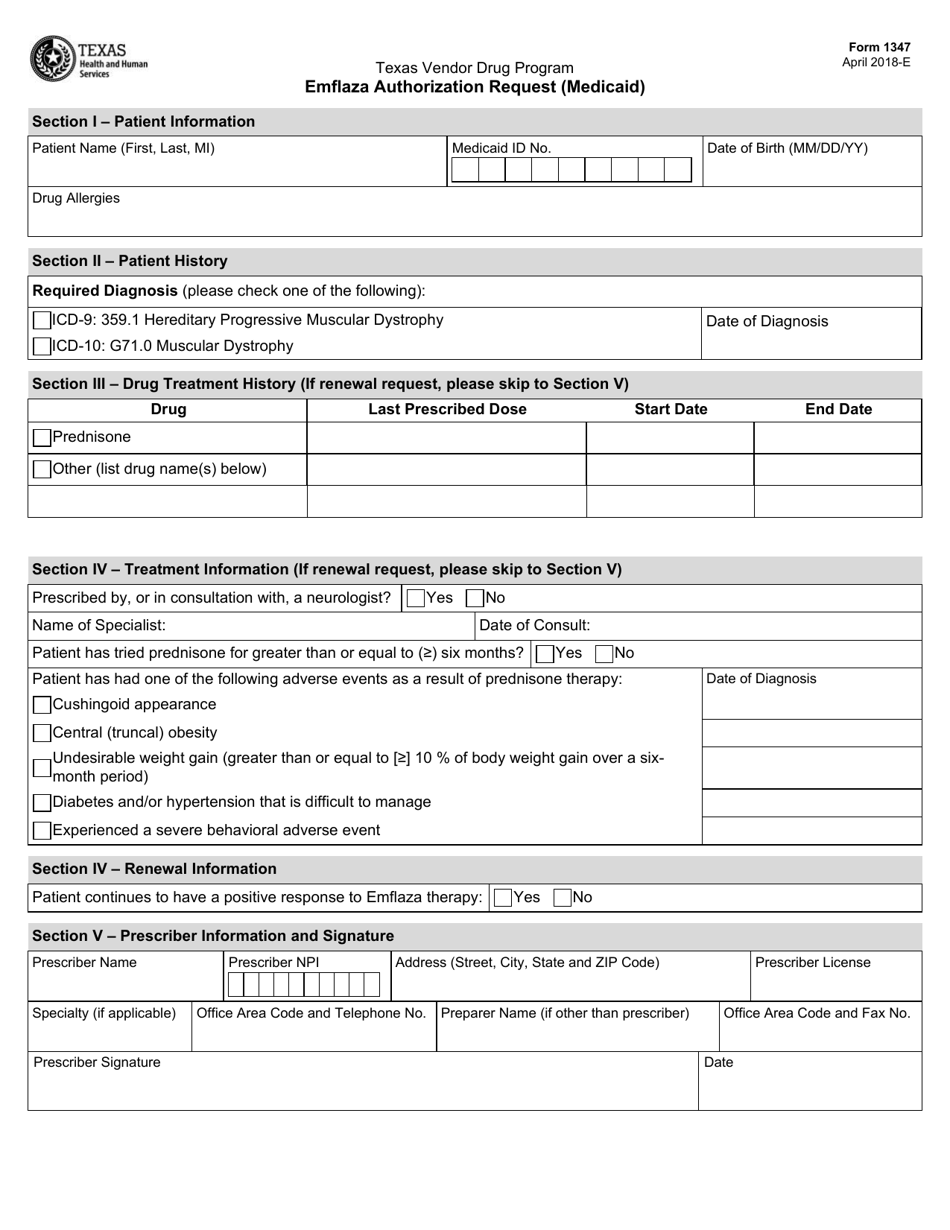
Form 1347 Emflaza Authorization Request (Medicaid) - Texas
What Is Form 1347?
This is a legal form that was released by the Texas Health and Human Services - a government authority operating within Texas. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is Form 1347 Emflaza Authorization Request?
A: Form 1347 Emflaza Authorization Request is a document used to request Medicaid coverage for the medication Emflaza in the state of Texas.
Q: What is Emflaza?
A: Emflaza is a medication used to treat Duchenne muscular dystrophy.
Q: Who can use Form 1347 Emflaza Authorization Request?
A: This form is for individuals who are eligible for Medicaid and need Medicaid coverage for Emflaza.
Q: What does Form 1347 Emflaza Authorization Request require?
A: The form requires information about the patient, their Medicaid eligibility, and the medical necessity for Emflaza.
Q: How long does it take to process Form 1347 Emflaza Authorization Request?
A: The processing time can vary, but it typically takes a few weeks to receive a decision on Medicaid coverage for Emflaza.
Q: Is there a cost for submitting Form 1347 Emflaza Authorization Request?
A: There is no cost for submitting the form, but Medicaid coverage for Emflaza may have certain cost-sharing requirements.
Q: Can I appeal if my Form 1347 Emflaza Authorization Request is denied?
A: Yes, if your request for Medicaid coverage for Emflaza is denied, you have the right to appeal the decision.
Q: Who can I contact for more information about Form 1347 Emflaza Authorization Request?
A: You can contact your local Medicaid office or the Texas Medicaid program for more information about the form and the Medicaid coverage for Emflaza.
Form Details:
- Released on April 1, 2018;
- The latest edition provided by the Texas Health and Human Services;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form 1347 by clicking the link below or browse more documents and templates provided by the Texas Health and Human Services.