![]() This version of the form is not currently in use and is provided for reference only. Download this version of
Form ODM03397
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
Form ODM03397
for the current year.
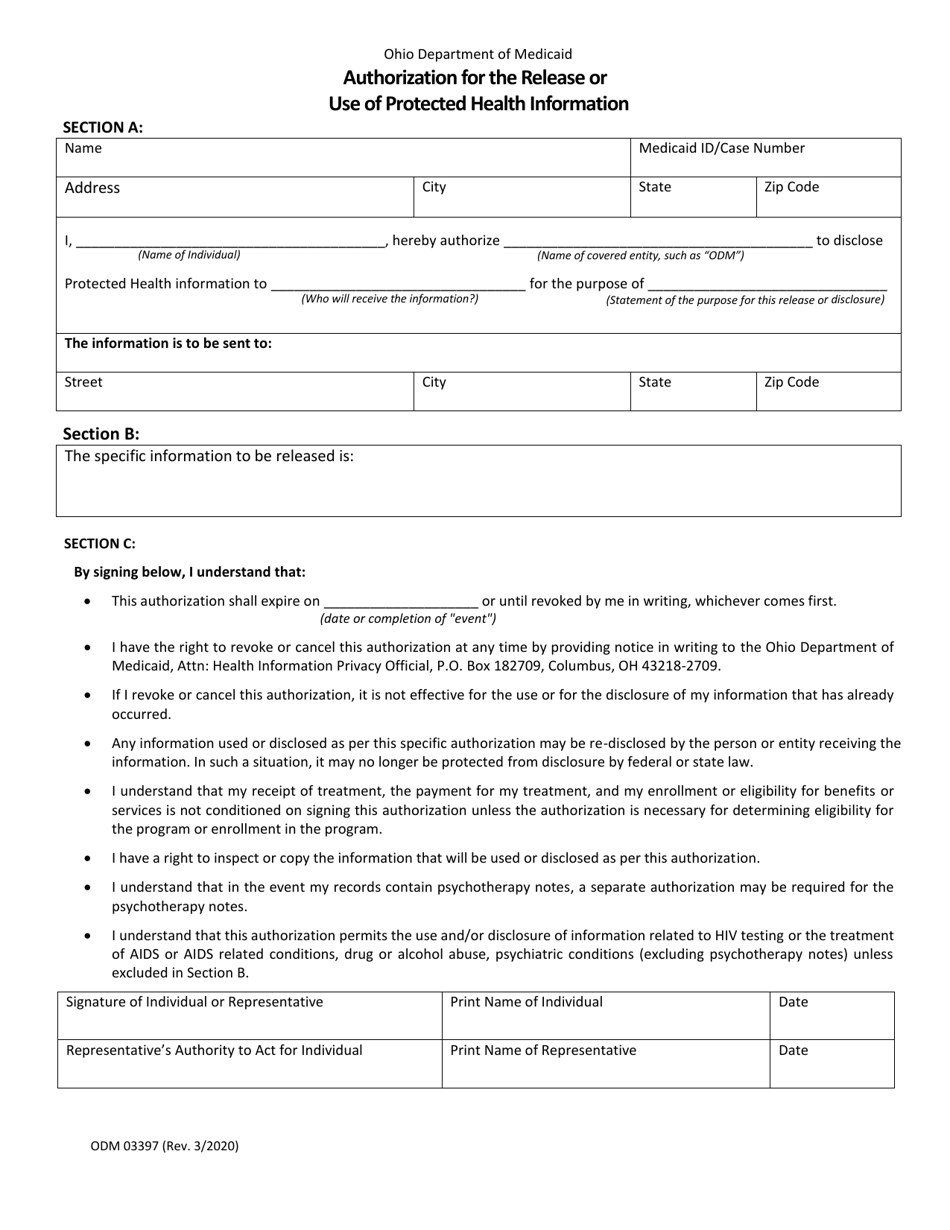
Form ODM03397 Authorization for the Release or Use of Protected Health Information - Ohio
What Is Form ODM03397?
This is a legal form that was released by the Ohio Department of Medicaid - a government authority operating within Ohio. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is ODM03397?
A: ODM03397 is a form used in Ohio to authorize the release or use of protected health information.
Q: Why would I need this form?
A: You may need this form to give permission for the release or use of your protected health information by a healthcare provider or other entity.
Q: What information is required on the form?
A: The form requires you to provide your personal information, specify the information to be released, indicate the purpose of the release, and provide your signature.
Q: Is this form specific to Ohio?
A: Yes, ODM03397 is specifically used in Ohio.
Q: Can I use this form for any healthcare provider?
A: Yes, you can use this form to authorize the release or use of your protected health information by any healthcare provider in Ohio.
Q: Is there a fee for using this form?
A: There is usually no fee for using ODM03397, but some healthcare providers may charge a small administrative fee.
Q: How long is this form valid?
A: The validity period of ODM03397 varies depending on the purpose of the release or use, but it is typically valid for one year.
Q: Can I revoke the authorization?
A: Yes, you can revoke the authorization at any time by notifying the healthcare provider or entity in writing.
Q: Are there any restrictions on the use of this form?
A: The use of ODM03397 is subject to state and federal laws governing the privacy and security of protected health information.
Form Details:
- Released on March 1, 2020;
- The latest edition provided by the Ohio Department of Medicaid;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form ODM03397 by clicking the link below or browse more documents and templates provided by the Ohio Department of Medicaid.