Application for Health Coverage & Help Paying Costs
The Application for Health Coverage & Help Paying Costs is a legal document used to apply for and enroll in Marketplace health coverage.
Alternate Names:
- Marketplace Application;
- Health Insurance Marketplace Application.
You can purchase health insurance via the Health Insurance Marketplace to obtain comprehensive coverage, lower your health coverage premiums, or sign up for Medicaid or the Children's Health Insurance Program (CHIP). Complete the Marketplace Application for yourself or any of your household members. The U.S. Department of Health and Human Services (DHHS) will receive your application and contact you within one-two weeks.
A fillable Application for Health Coverage can be downloaded through the link below.
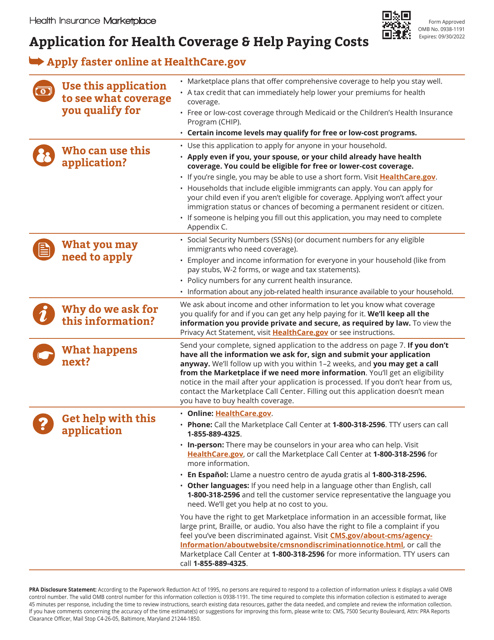
How to Fill Out Application for Health Coverage & Help Paying Costs?
An Application for Health Coverage & Help Paying Costs instructions are as follows:
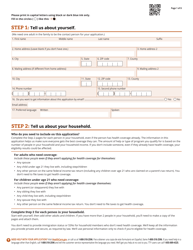
- Provide your personal details - full name, residential and mailing addresses, telephone numbers, email address, and preferred language;
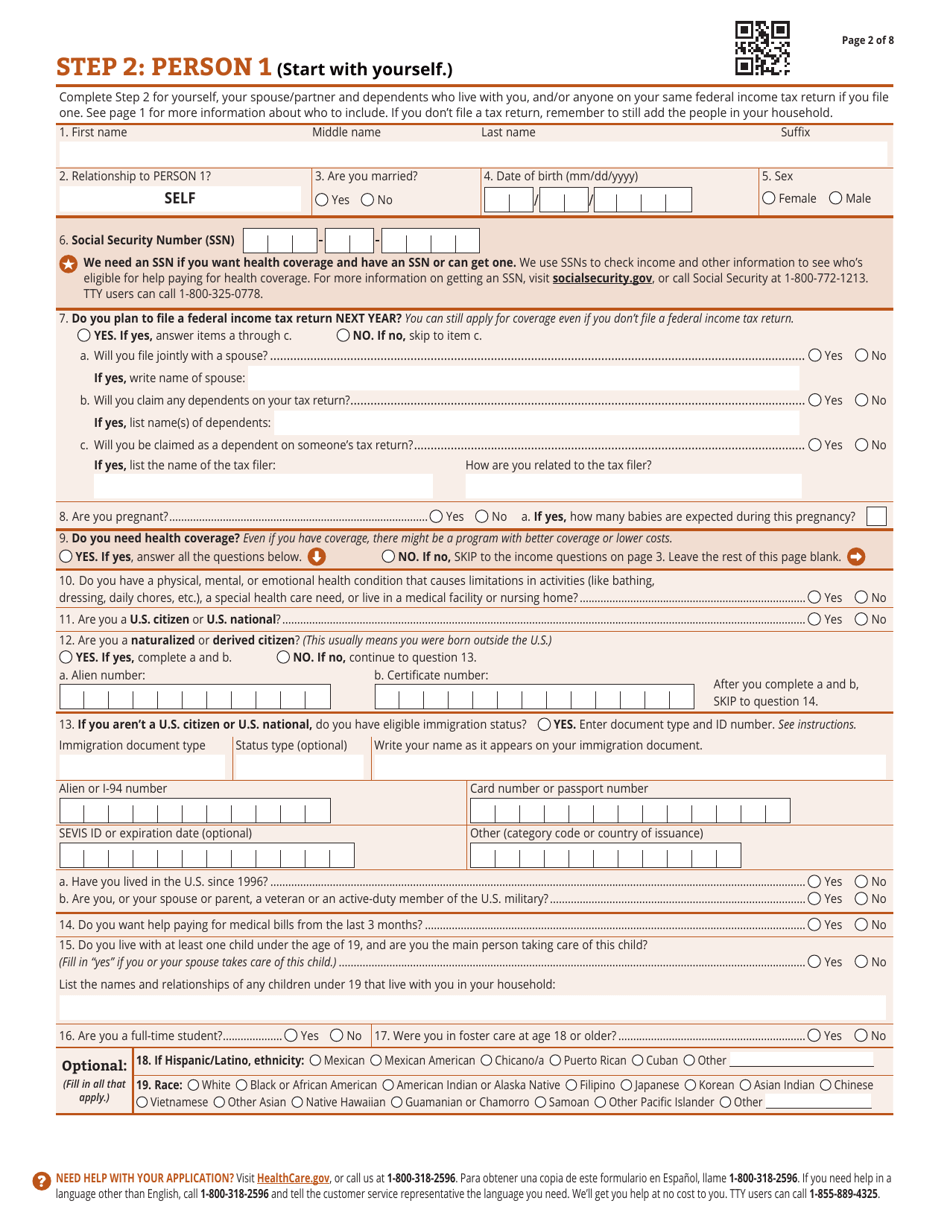
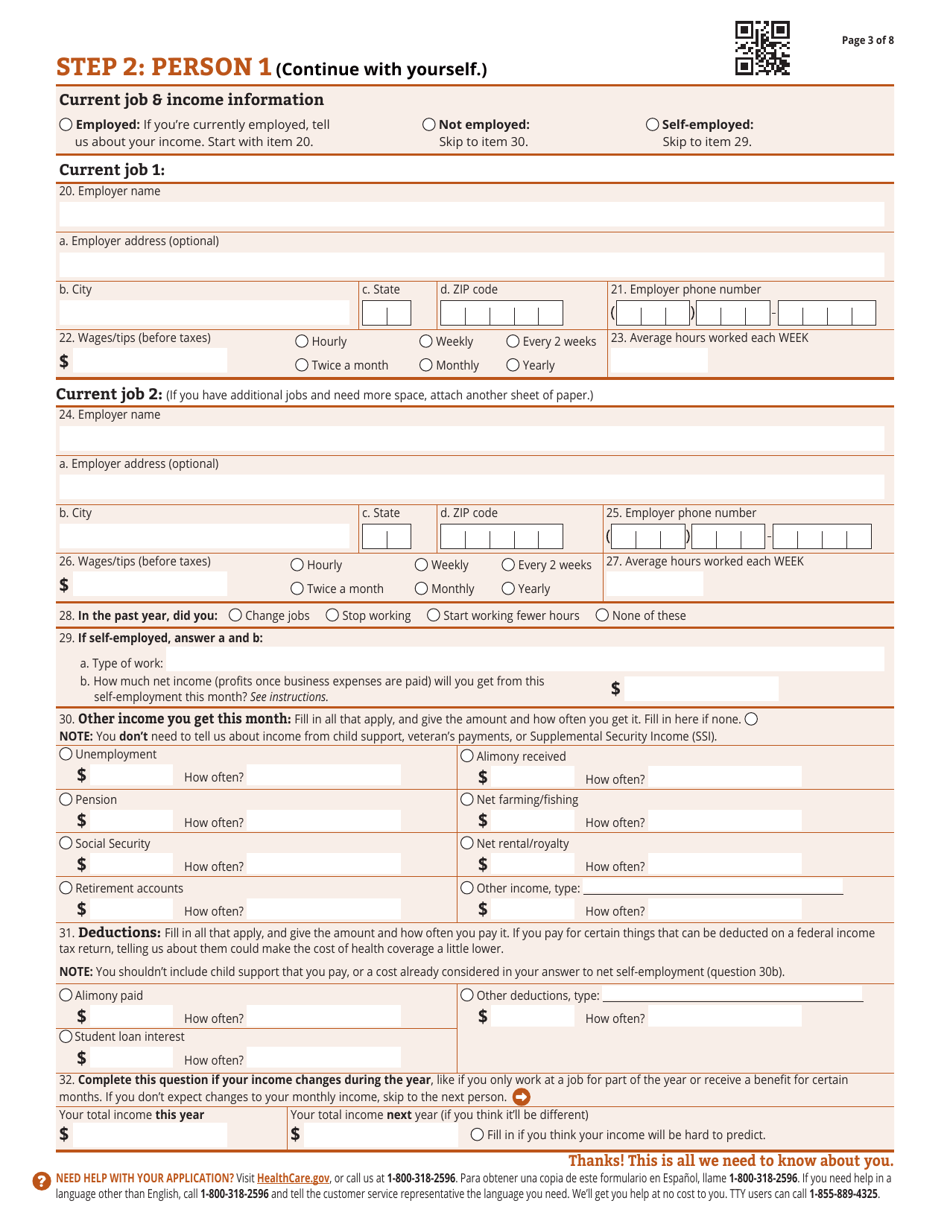
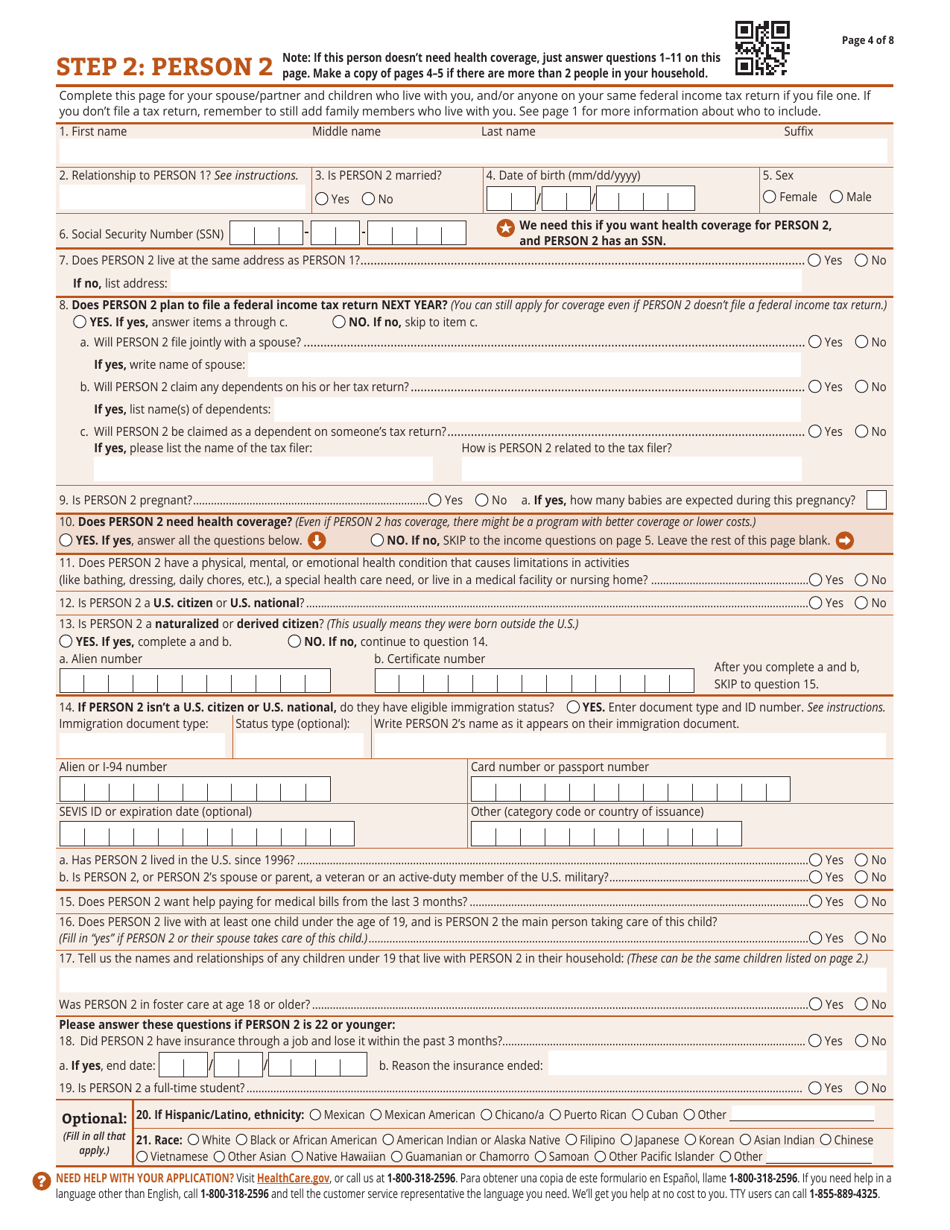
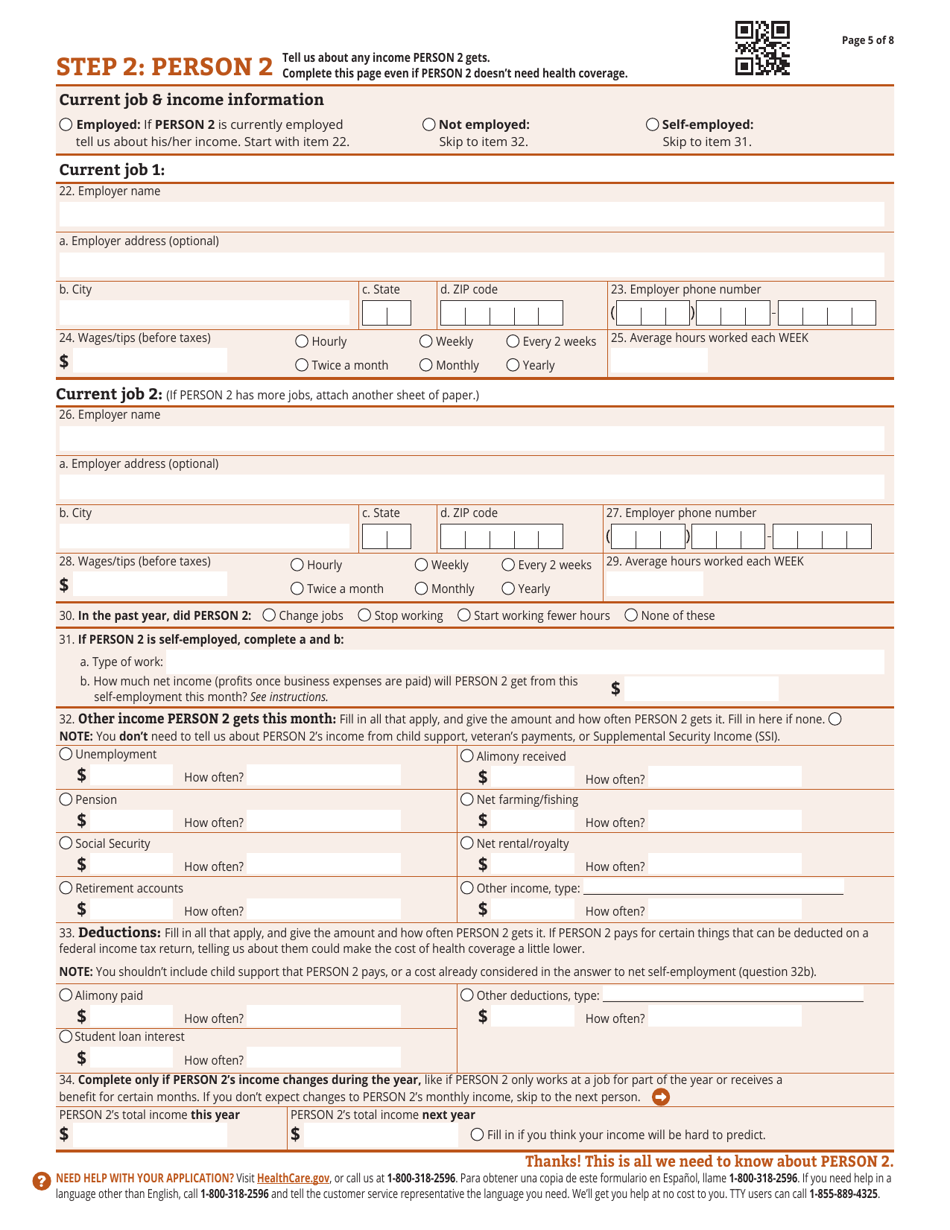
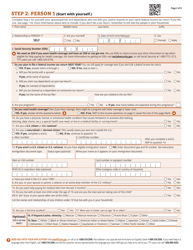
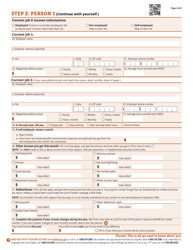
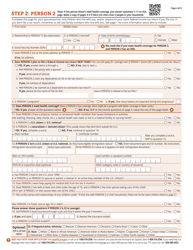
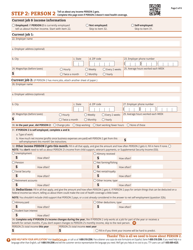
- Include the details of every individual in your household starting with yourself. You will have to indicate the names of the household members, their marriage status, dates of birth, sexes, social security numbers, and addresses. State whether the household members plan to file an income tax return next year and whether they need health coverage. Indicate their citizenship or immigration status. Write down the employment history of each individual and describe their sources of income;
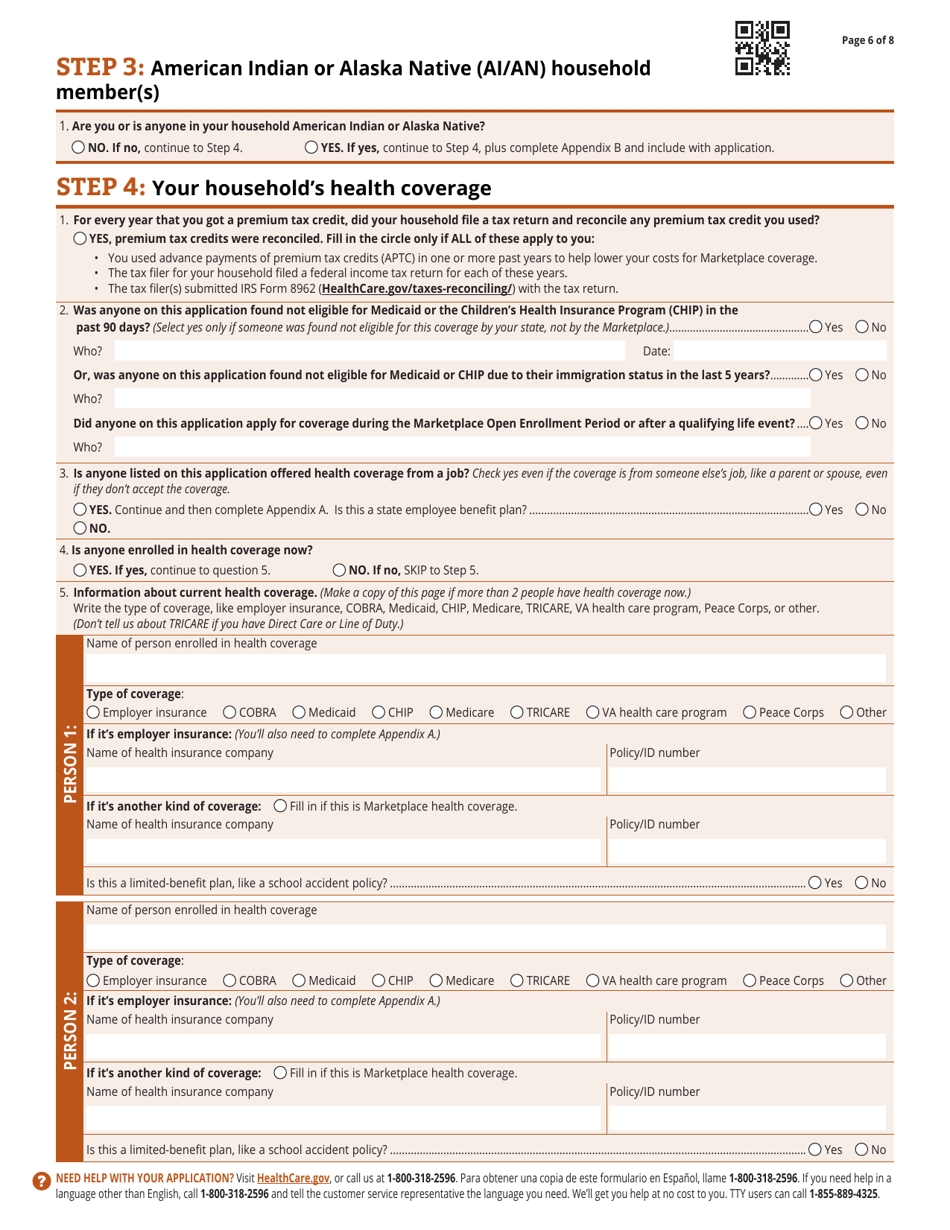
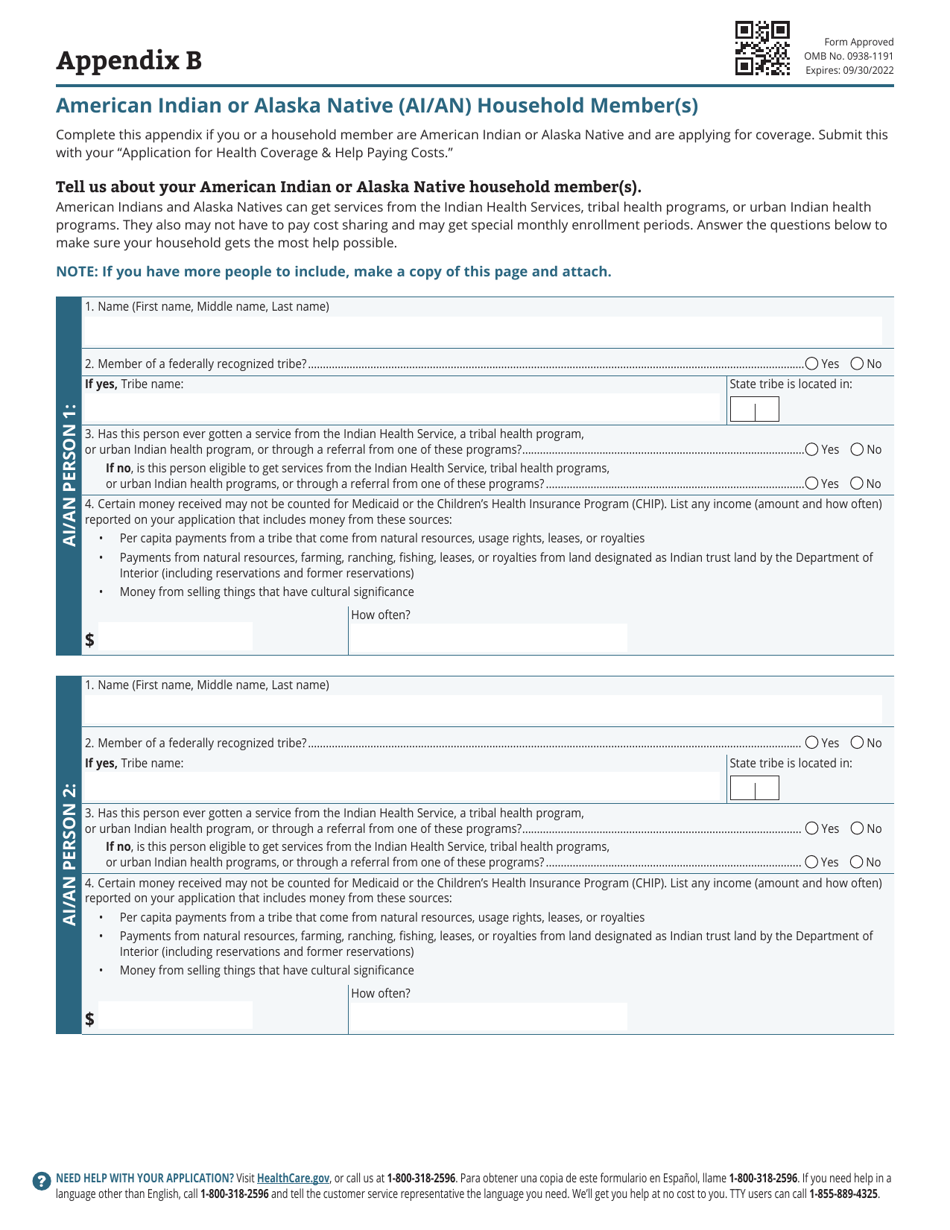
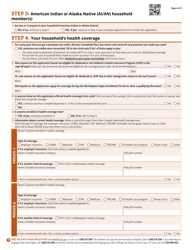
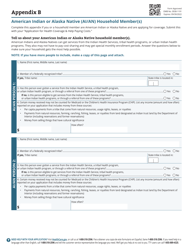
- Check the appropriate box if anyone in your household is Alaska Native or American Indian. Additionally, complete Appendix B - indicate the name of the individual and the tribe name, and state whether the individual received any help from a tribal or urban health program;
- Provide information about your current health coverage. State whether anyone on the application was found not eligible for Medicaid or CHIP and is anyone enrolled in health coverage now. Record the type of coverage your household members have;
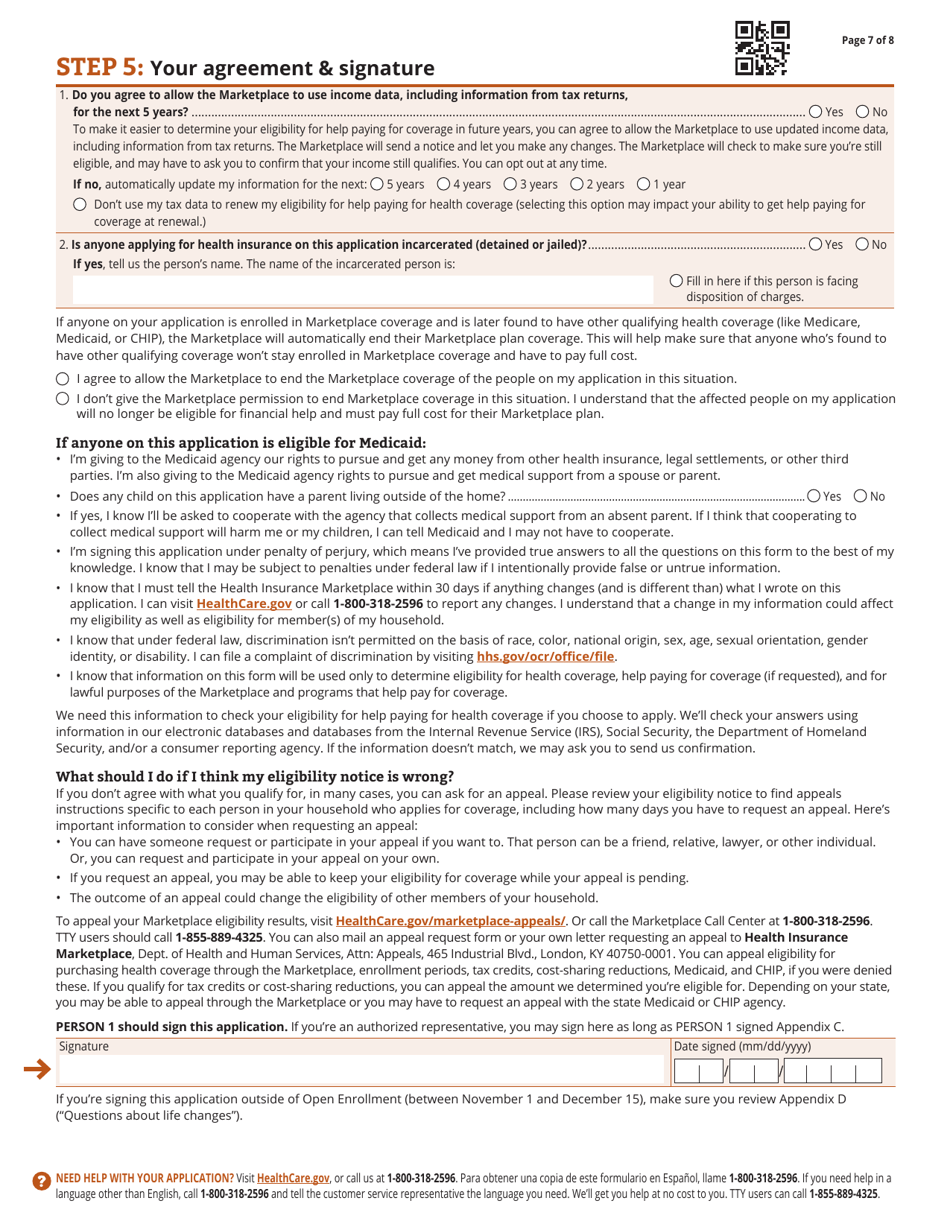
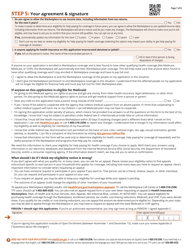
- Allow the Marketplace to process your data. If anyone on the application is currently incarcerated, enter this individual's name. Sign and date the form;
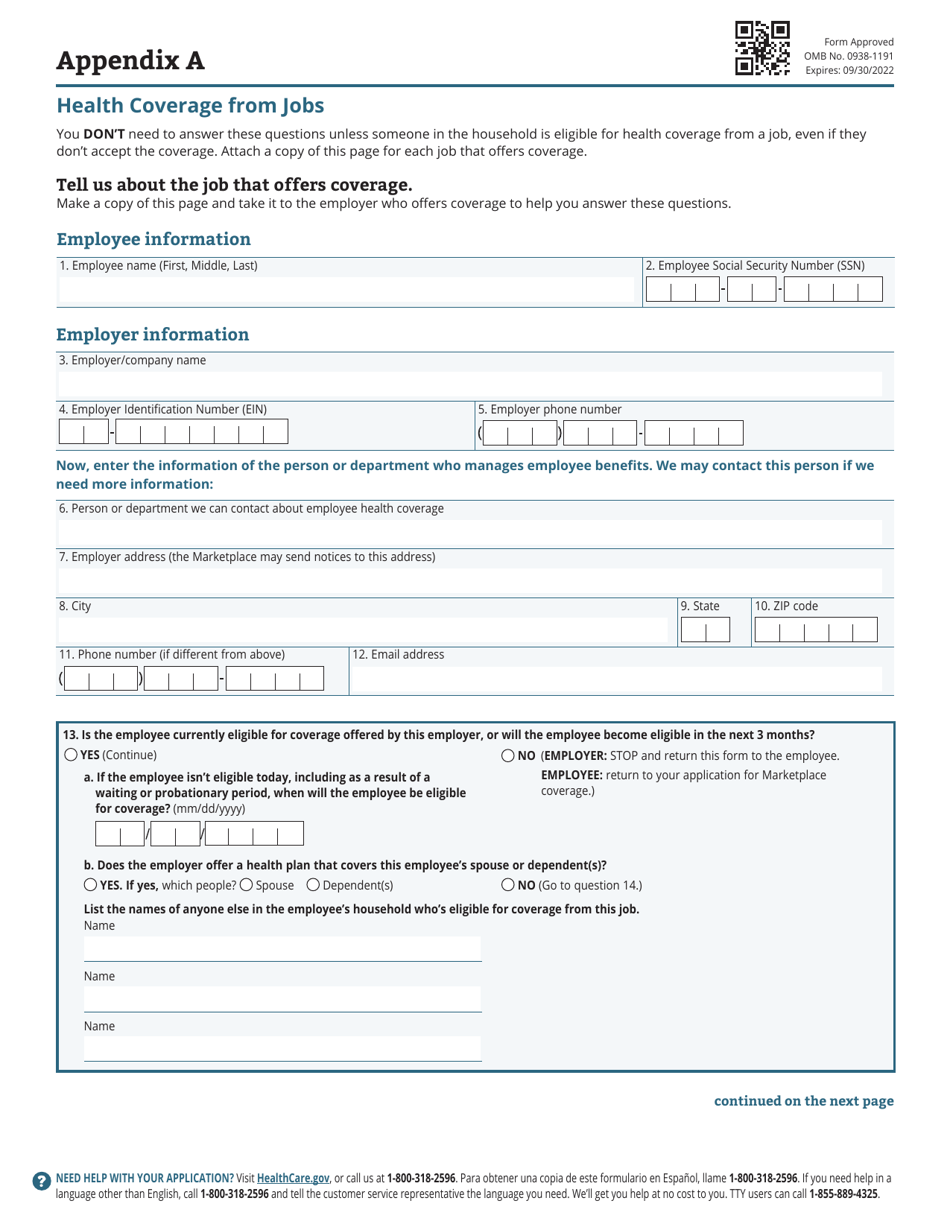
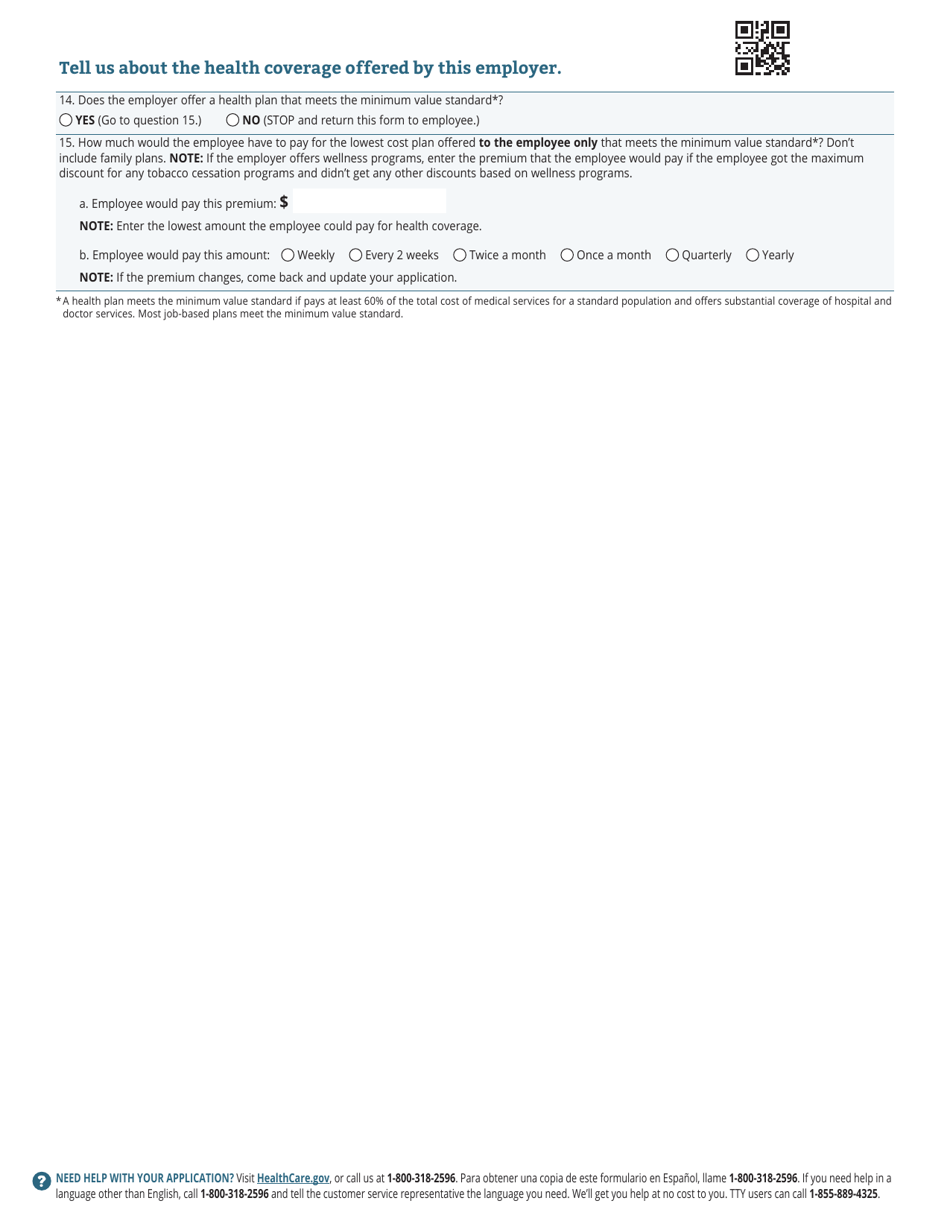
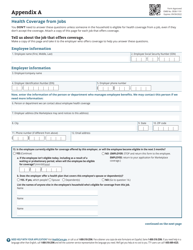
- Complete Appendix A if a household member qualifies for health coverage from a job. Add the employee and employer's details, record the name of the individual or department that manages employee benefits, and describe the health plan offered by the employer;
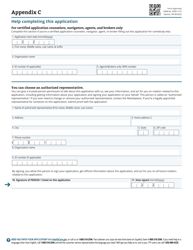
- Complete Appendix C if you are filing the application for someone else as their personal representative to provide your personal details. Also, you may appoint a trusted individual as your authorized representative by indicating their details using this Appendix;
- Complete Appendix D if anyone on the application has experienced or will experience life changes in the past or next 60 days - marriage, losing health coverage, release from incarceration, etc.
Once you prepare the application, send it to the Health Insurance Marketplace, Dept. of Health and Human Services, 465 Industrial Blvd., London, KY 40750-0001.
Related Templates and Forms:
Download Application for Health Coverage & Help Paying Costs

1
2
3
4
5
6
7
8

9

10
11

12
13
14

15