Form DHS-6340-ENG Other Health Insurance Reporting Form - Minnesota
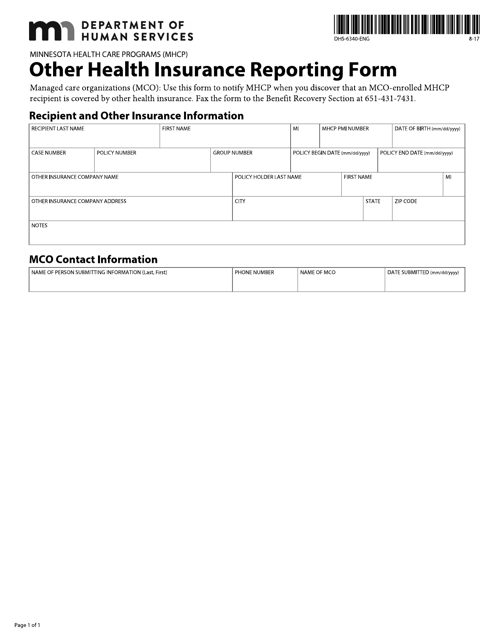
What Is Form DHS-6340-ENG?
This is a legal form that was released by the Minnesota Department of Human Services - a government authority operating within Minnesota. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is Form DHS-6340-ENG?
A: Form DHS-6340-ENG is the Other Health Insurance Reporting Form.
Q: Who is required to fill out Form DHS-6340-ENG?
A: Residents of Minnesota who have other health insurance coverage are required to fill out this form.
Q: Why do I need to fill out Form DHS-6340-ENG?
A: You need to fill out this form to report any other health insurance coverage you have.
Q: When is the deadline to submit Form DHS-6340-ENG?
A: The deadline to submit this form is determined by the Minnesota Department of Human Services, and it may vary from year to year.
Q: What happens if I don't fill out Form DHS-6340-ENG?
A: Failure to fill out this form accurately and on time may result in consequences such as loss of benefits or penalties.
Q: Are there any exemptions from filling out Form DHS-6340-ENG?
A: There may be exemptions for certain individuals, such as those who are eligible for public health care programs.
Q: What information do I need to fill out Form DHS-6340-ENG?
A: You will need to provide information about your other health insurance coverage, such as the policy number and coverage period.
Q: Is Form DHS-6340-ENG confidential?
A: Yes, the information provided on this form is confidential and will only be used for the purpose of determining eligibility for health care programs.
Form Details:
- Released on August 1, 2017;
- The latest edition provided by the Minnesota Department of Human Services;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form DHS-6340-ENG by clicking the link below or browse more documents and templates provided by the Minnesota Department of Human Services.