Form HFS2305A Air Fluidized Bed Questionnaire - Illinois
What Is Form HFS2305A?
This is a legal form that was released by the Illinois Department of Healthcare and Family Services - a government authority operating within Illinois. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
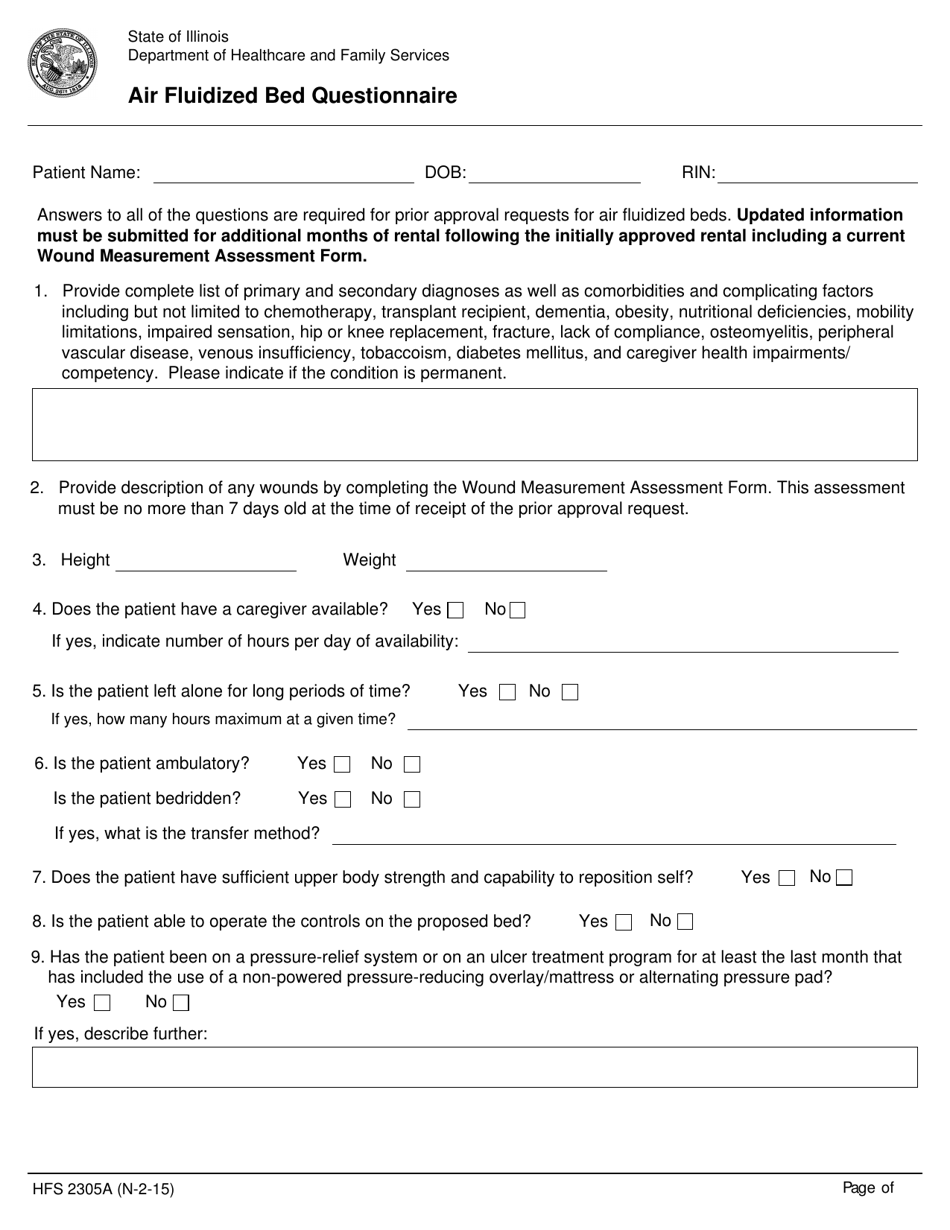
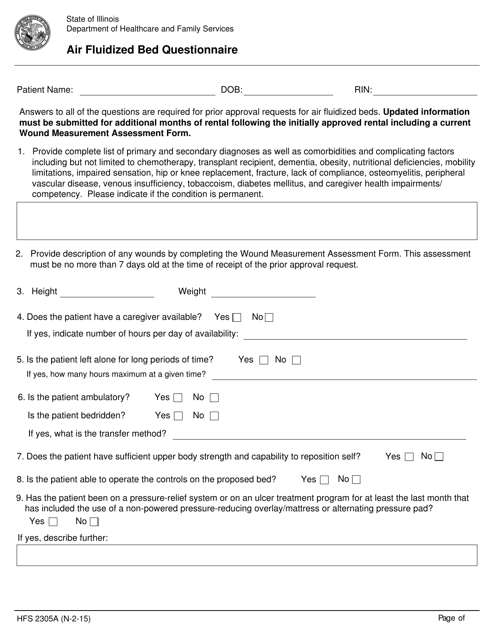
Q: What is the purpose of Form HFS2305A Air Fluidized Bed Questionnaire?
A: The purpose of Form HFS2305A Air Fluidized Bed Questionnaire is to collect information about individuals who require air fluidized bed therapy in Illinois.
Q: Who needs to complete Form HFS2305A Air Fluidized Bed Questionnaire?
A: The questionnaire needs to be completed by individuals who require air fluidized bed therapy in Illinois.
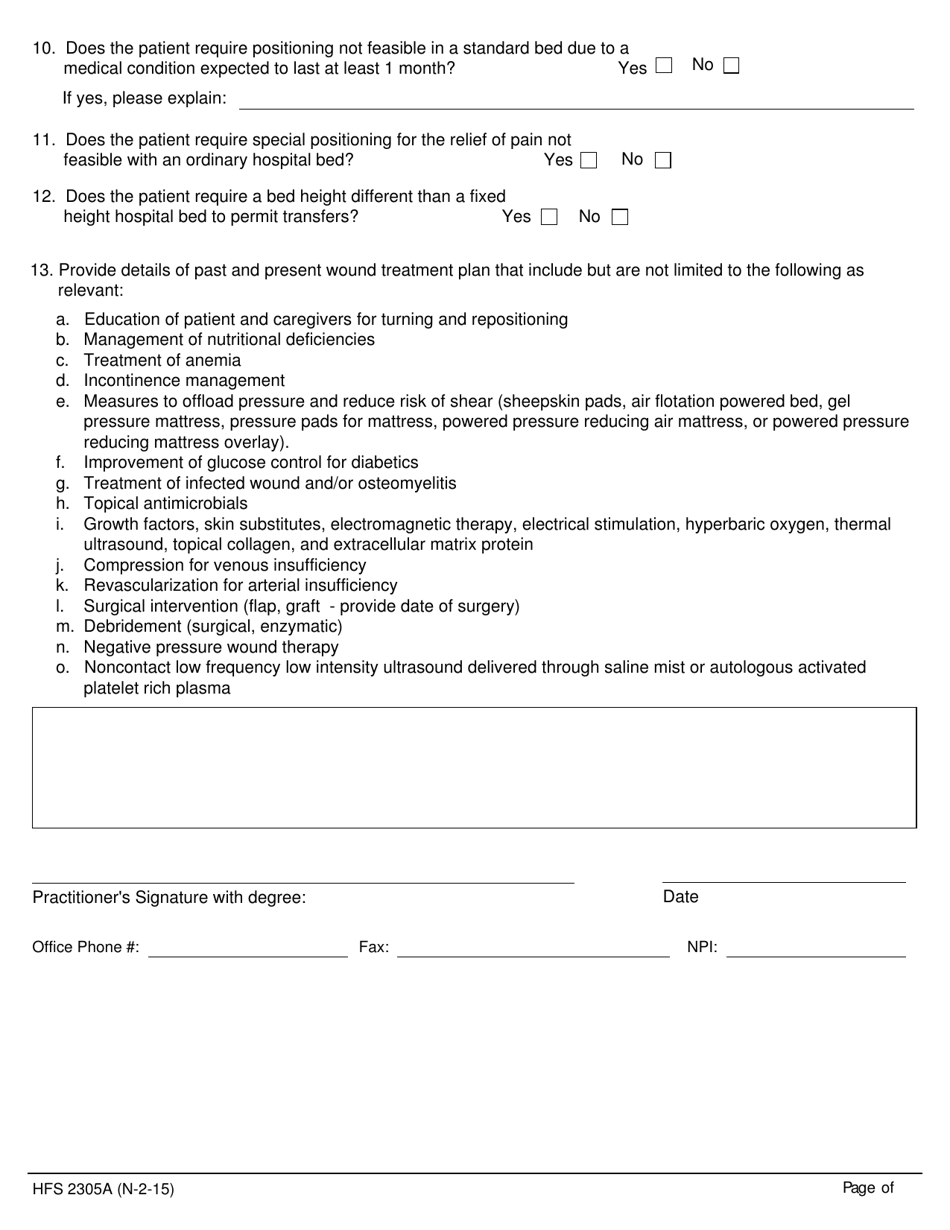
Q: What information is required in Form HFS2305A Air Fluidized Bed Questionnaire?
A: The questionnaire requires information such as the individual's name, address, date of birth, medical condition, and the reason for needing air fluidized bed therapy.
Q: Is the completion of Form HFS2305A Air Fluidized Bed Questionnaire mandatory?
A: Yes, the completion of Form HFS2305A Air Fluidized Bed Questionnaire is mandatory for individuals who require air fluidized bed therapy in Illinois.
Form Details:
- Released on February 1, 2015;
- The latest edition provided by the Illinois Department of Healthcare and Family Services;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form HFS2305A by clicking the link below or browse more documents and templates provided by the Illinois Department of Healthcare and Family Services.
Download Form HFS2305A Air Fluidized Bed Questionnaire - Illinois
1
2